Primary and Community Care Department Nijmegen, Radboud University Medical Center, Nijmegen, The Netherlands.
Zorggroep Onze Huisartsen, Arnhem, the Netherlands.
Sci Rep. 2024 May 29;14(1):12367. doi: 10.1038/s41598-024-62349-9.
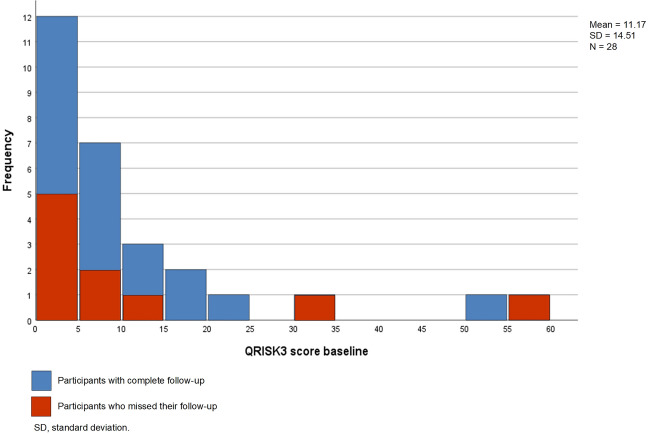
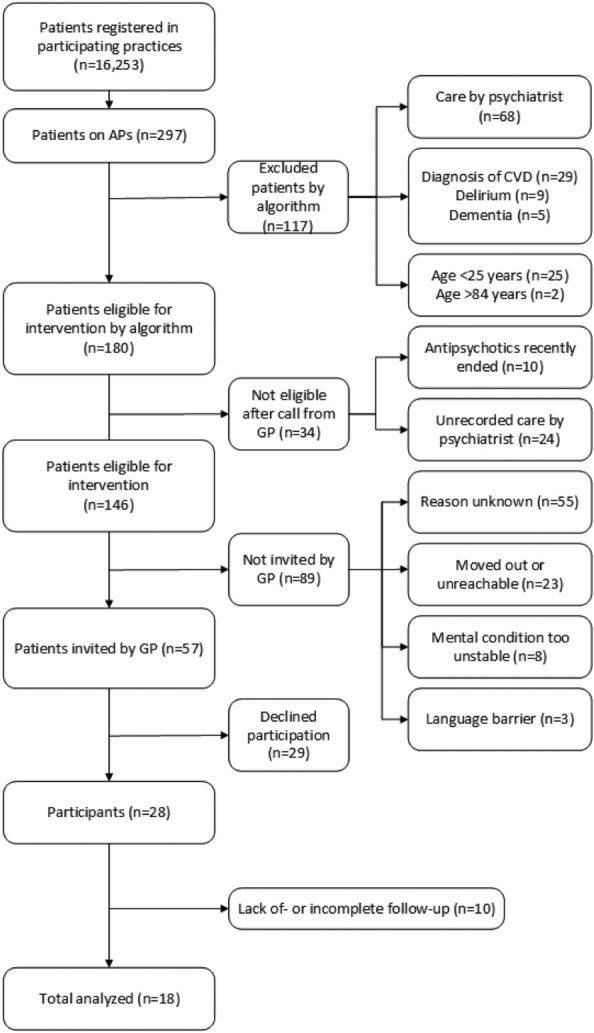
General practitioners (GPs) are often unaware of antipsychotic (AP)-induced cardiovascular risk (CVR) and therefore patients using atypical APs are not systematically monitored. We evaluated the feasibility of a complex intervention designed to review the use of APs and advise on CVR-lowering strategies in a transmural collaboration. A mixed methods prospective cohort study in three general practices in the Netherlands was conducted in 2021. The intervention comprised three steps: a digital information meeting, a multidisciplinary meeting, and a shared decision-making visit to the GP. We assessed patient recruitment and retention rates, advice given and adopted, and CVR with QRISK3 score and mental state with MHI-5 at baseline and three months post-intervention. GPs invited 57 of 146 eligible patients (39%), of whom 28 (19%) participated. The intervention was completed by 23 (82%) and follow-up by 18 participants (64%). At the multidisciplinary meeting, 22 (78%) patients were advised to change AP use. Other advice concerned medication (other than APs), lifestyle, monitoring, and psychotherapy. At 3-months post-intervention, 41% (28/68) of this advice was adopted. Our findings suggest that this complex intervention is feasible for evaluating health improvement in patients using AP in a trial.
全科医生(GP)通常不了解抗精神病药(AP)引起的心血管风险(CVR),因此,使用非典型 AP 的患者并未进行系统监测。我们评估了一项复杂干预措施的可行性,该措施旨在在跨领域合作中审查 AP 的使用情况,并就降低 CVR 的策略提供建议。这是一项于 2021 年在荷兰的三家全科诊所开展的混合方法前瞻性队列研究。该干预措施包括三个步骤:数字信息会议、多学科会议以及与全科医生进行共同决策访问。我们评估了患者的招募和保留率、提供和采纳的建议以及使用 QRISK3 评分评估的 CVR 和使用 MHI-5 评估的精神状态,基线和干预后三个月分别进行评估。GP 邀请了 146 名符合条件的患者中的 57 名(39%),其中 28 名(19%)参与。23 名(82%)完成了干预,18 名(64%)完成了随访。在多学科会议上,建议 22 名(78%)患者改变 AP 的使用。其他建议涉及药物(AP 以外的药物)、生活方式、监测和心理治疗。在干预后 3 个月,该建议的采纳率为 41%(28/68)。我们的研究结果表明,对于在试验中评估使用 AP 的患者的健康改善,该复杂干预措施是可行的。