Mortsiefer Achim, Meysen Tobias, Schumacher Martin, Abholz Heinz-Harald, Wegscheider Karl, In der Schmitten Jürgen
Institute of General Medicine, Medical Faculty, Heinrich-Heine-University Düsseldorf, P.O. Box 101001, 40225, Düsseldorf, Germany.
Department of Medical Biometry and Epidemiology, University Medical Center Hamburg-Eppendorf, Martinistrasse 52, 20246, Hamburg, Germany.
BMC Fam Pract. 2015 May 7;16:56. doi: 10.1186/s12875-015-0274-1.
Guidelines on hypertension management recommend adjusting therapeutic efforts in accordance with global cardiovascular risk (CVR) rather than by blood pressure levels alone. However, this paradigm change has not yet arrived in German General Practice. We have evaluated the effect of an educational outreach visit with general practitioners (GPs), encouraging them to consider CVR in treatment decisions for patients with hypertension.
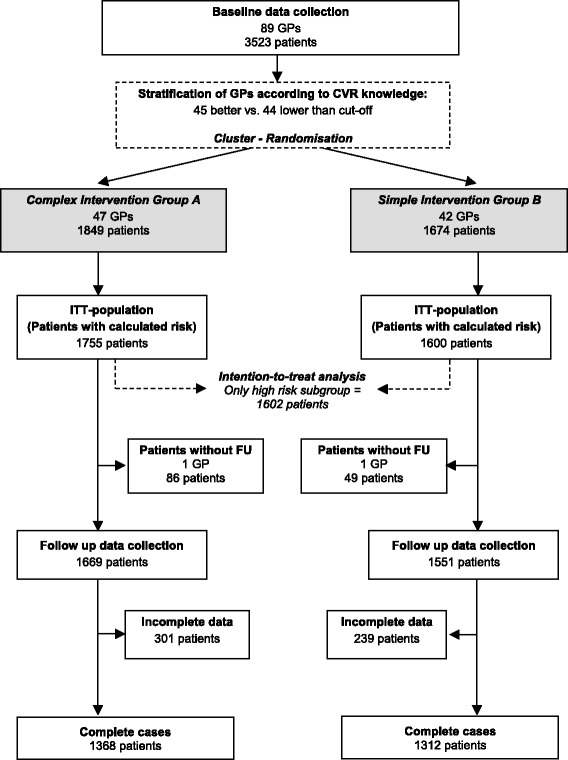
Prospective cluster-randomised trial comprising 3443 patients with known hypertension treated by 87 GPs. Practices were randomly assigned to complex (A) or simple (B) intervention. Both groups received a guideline by mail; group A also received complex peer intervention promoting the concept of global CVR. Clinical data were collected at baseline and 6-9 months after intervention. Main outcome was improvement of calculated CVR in the predefined subpopulation of patients with a high CVR (10-year mortality ≥5%), but no manifest cardiovascular disease.
Adjusted for baseline the follow-up CVR were 13.1% (95% CI 12.6%-13.6%) (A) and 12.6% (95% CI 12.2%-13.1%) (B) with a group difference (A vs. B) of 0.5% (-0.2%-1.1%), p = 0.179. The group difference was -0.05% in patients of GPs familiar with global CVR and 1.1% in patients of GPs not familiar with with global CVR. However, this effect modification was not significant (p = 0.165). Pooled over groups, the absolute CVR reduction from baseline was 1.0%, p < 0.001. The ICC was 0.026 (p = 0.002). Hypertension control (BP <140/90 mmHg) improved in the same subpopulation from 38.1 to 45.9% in the complex intervention group, and from 35.6 to 46.5% in the simple intervention group, with adjusted follow-up control rates of 46.7% (95% CI 40.4%-53.1%) (A) and 46.9% (95% CI 40.3%-53.5% (B) and an adjusted odds ratio (A vs B) of 0.99 (95% CI 0.68-1.45), p = 0.966.
Our complex educational intervention, including a clinical outreach visit, had no significant effect on CVR of patients with known hypertension at high risk compared to a simple postal intervention.
ISRCTN44478543 .
高血压管理指南建议根据全球心血管风险(CVR)而非仅依据血压水平来调整治疗措施。然而,这种范式转变在德国全科医疗中尚未实现。我们评估了一次针对全科医生(GP)的教育推广访问的效果,鼓励他们在高血压患者的治疗决策中考虑CVR。
前瞻性整群随机试验,纳入了由87名全科医生治疗的3443例已知高血压患者。诊所被随机分配至复杂干预组(A)或简单干预组(B)。两组均通过邮件收到一份指南;A组还接受了促进全球CVR概念的复杂同伴干预。在基线和干预后6 - 9个月收集临床数据。主要结局是在预先定义的高CVR(10年死亡率≥5%)但无明显心血管疾病的患者亚组中,计算得出的CVR有所改善。
校正基线后,随访时A组的CVR为13.1%(95%CI 12.6% - 13.6%),B组为12.6%(95%CI 12.2% - 13.1%),组间差异(A组对比B组)为0.5%(-0.2% - 1.1%),p = 0.179。在熟悉全球CVR的全科医生的患者中,组间差异为 - 0.05%,在不熟悉全球CVR的全科医生的患者中为1.1%。然而,这种效应修饰并不显著(p = 0.165)。合并两组来看,CVR较基线的绝对降低为1.0%,p < 0.001。组内相关系数(ICC)为0.026(p = 0.002)。在同一亚组中,复杂干预组的高血压控制(血压<140/90 mmHg)从38.1%提高到45.9%,简单干预组从35.6%提高到46.5%,校正后的随访控制率分别为46.7%(95%CI 40.4% - 53.1%)(A组)和46.9%(95%CI 40.3% - 53.5%)(B组),校正后的优势比(A组对比B组)为0.99(95%CI 0.68 - 1.45),p = 0.966。
与简单的邮寄干预相比,我们包括临床推广访问在内的复杂教育干预对已知高血压高危患者的CVR没有显著影响。
ISRCTN44478543