Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, USA.
Department of Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH, USA.
Eur J Heart Fail. 2024 Jul;26(7):1642-1651. doi: 10.1002/ejhf.3302. Epub 2024 Jun 4.
Patients with pulmonary hypertension (PH) are grouped based upon clinical and haemodynamic characteristics. Groups 2 (G2, left heart disease [LHD]) and 3 (G3, lung disease or hypoxaemia) are most common. Many patients display overlapping characteristics of heart and lung disease (G2-3), but this group is not well-characterized.
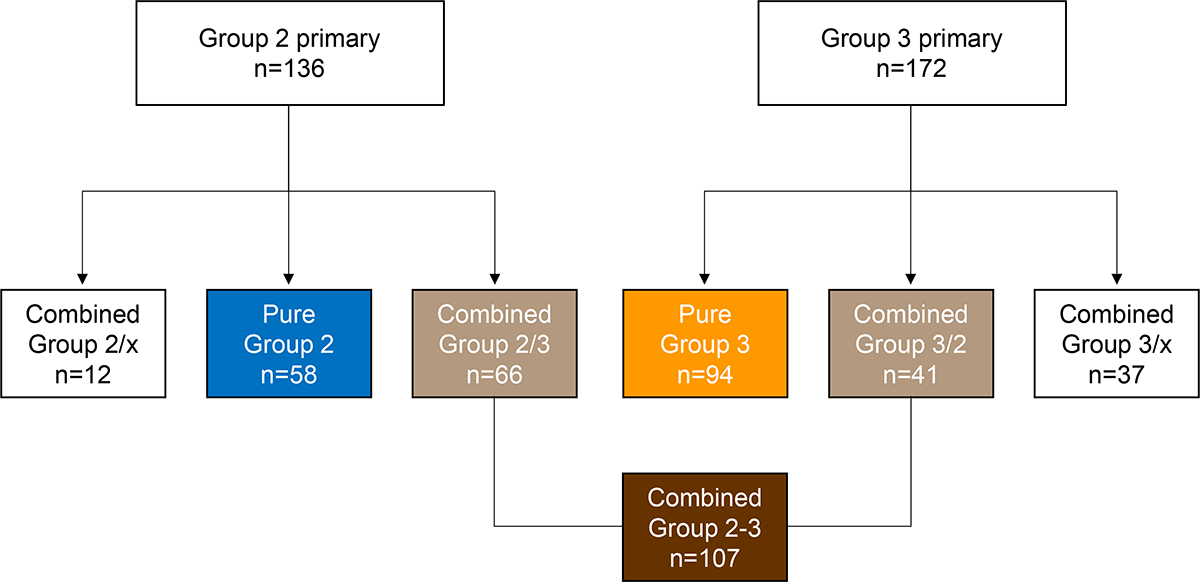
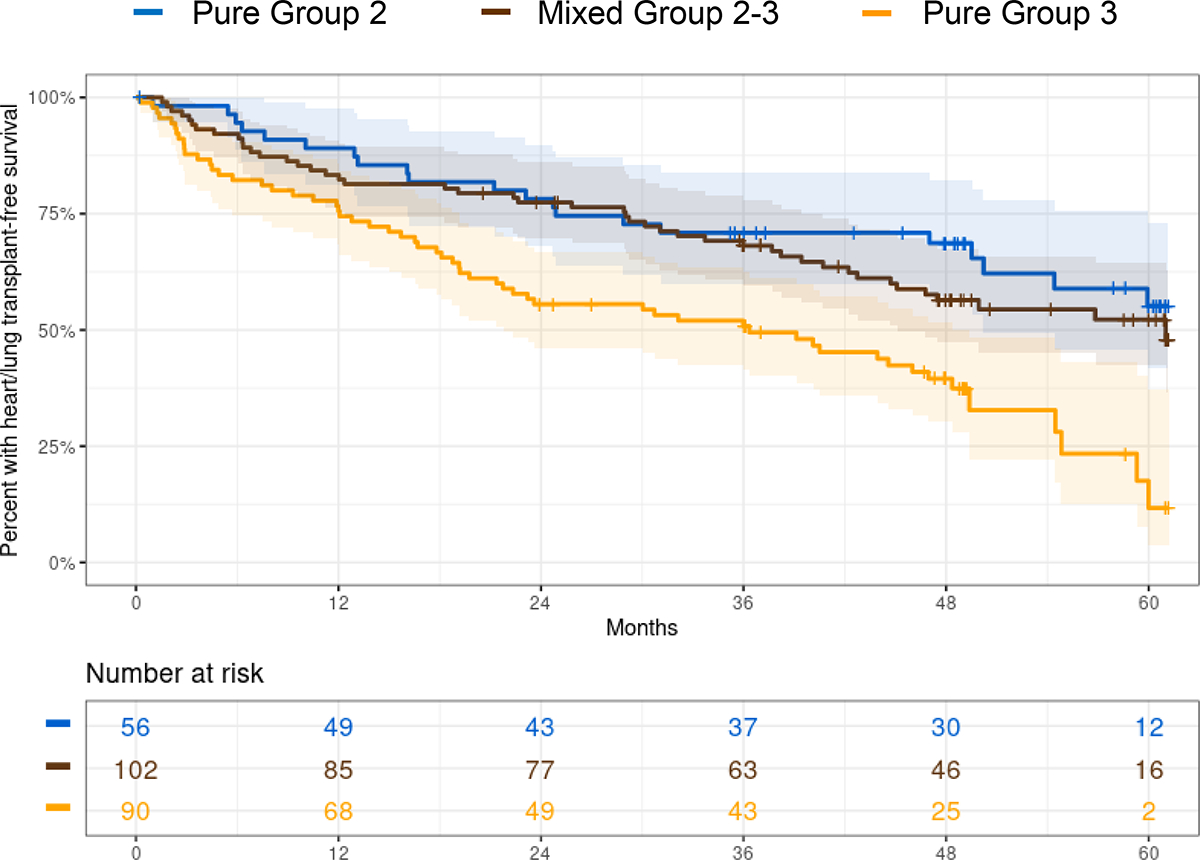
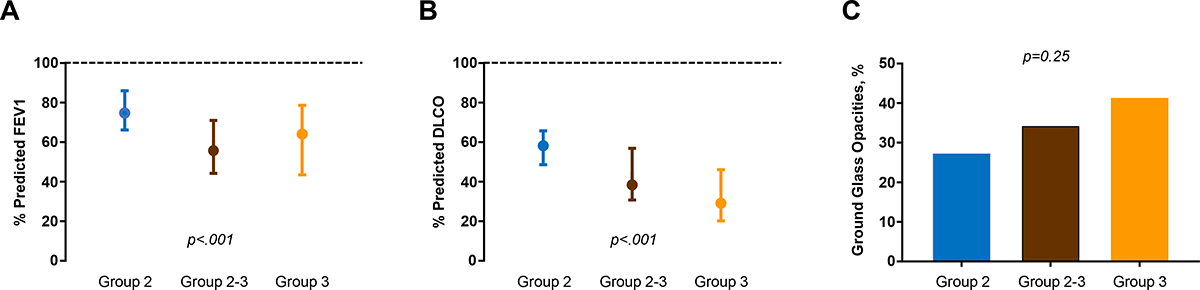
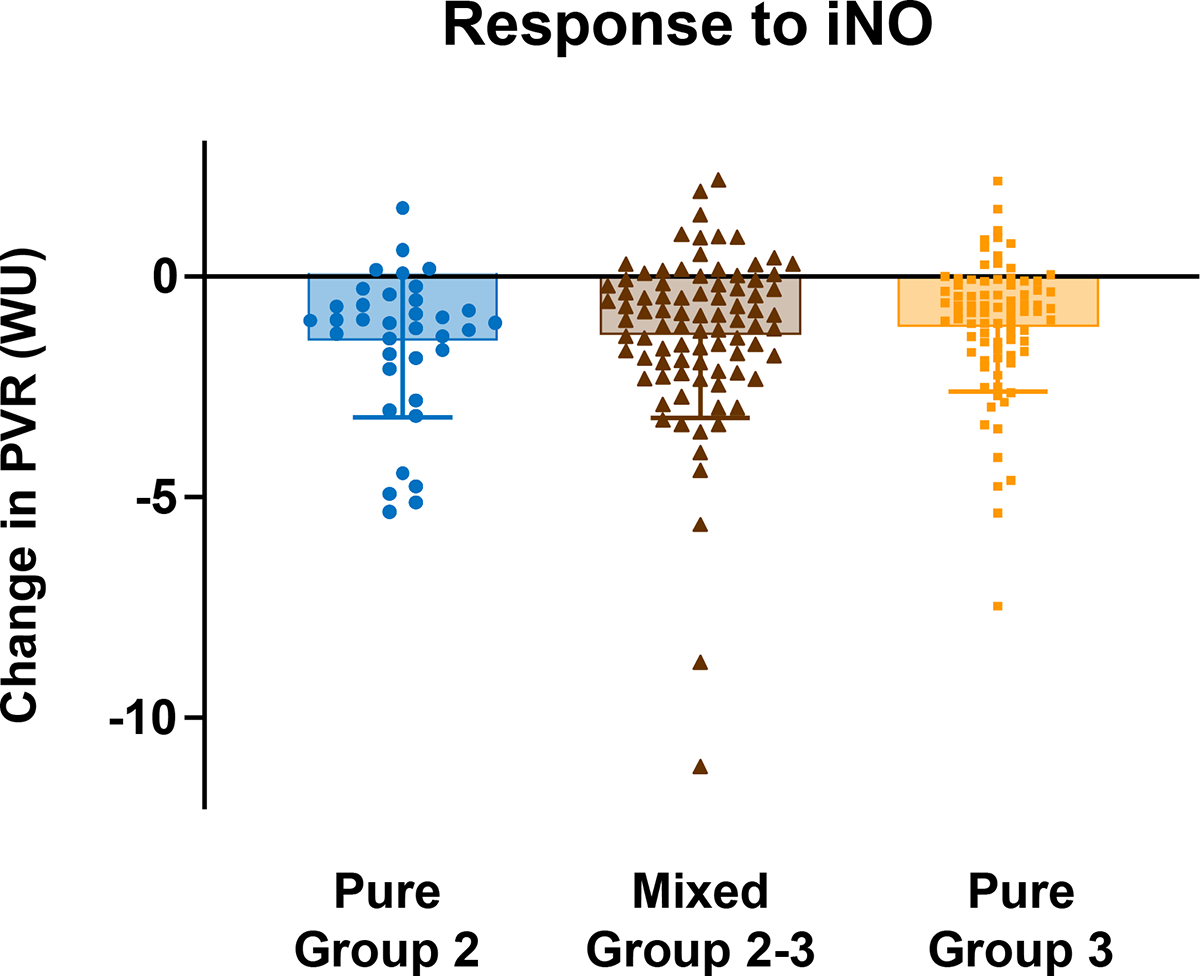
Patients with PH enrolled in the prospective, NHLBI-sponsored PVDOMICS network underwent intensive clinical, biomarker, imaging, gas exchange and exercise phenotyping. Patients with pure G2, pure G3, or overlapping G2-3 PH were compared across multiple phenotypic domains. Of all patients with predominant G2 (n = 136), 66 (49%) were deemed to have secondary lung disease/hypoxaemia contributors (G2/3), and of all patients categorized as predominant G3 (n = 172), 41 (24%) were judged to have a component of secondary LHD (G3/2), such that 107 had G2-3 (combined G2/3 and G3/2). As compared with G3, patients with G2 and G2-3 were more obese and had greater prevalence of hypertension, atrial fibrillation, and coronary disease. Patients with G2 and G2-3 were more anaemic, with poorer kidney function, more cardiac dysfunction, and higher N-terminal pro-B-type natriuretic peptide than G3. Lung diffusion was more impaired in G3 and G2-3, but commonly abnormal even in G2. Exercise capacity was severely and similarly impaired across all groups, with no differences in 6-min walk distance or peak oxygen consumption, and pulmonary vasoreactivity to nitric oxide did not differ. In a multivariable Cox regression model, patients with G2 had lower risk of death or transplant compared with G3 (hazard ratio [HR] 0.51, 95% confidence interval [CI] 0.30-0.86), and patients with G2-3 also displayed lower risk compared with G3 (HR 0.57, 95% CI 0.38-0.86).
Overlap is common in patients with a pulmonary or cardiac basis for PH. While lung structure/function is clearly more impaired in G3 and G2-3 than G2, pulmonary abnormalities are common in G2, even when clinically judged as isolated LHD. Further study is required to identify optimal systematic evaluations to guide therapeutic innovation for PH associated with combined heart and lung disease.
ClinicalTrials.gov NCT02980887.
肺动脉高压(PH)患者根据临床和血流动力学特征进行分组。第 2 组(G2,左心疾病[LHD])和第 3 组(G3,肺部疾病或低氧血症)最为常见。许多患者表现出心脏和肺部疾病的重叠特征(G2-3),但该组尚未得到很好的描述。
参与前瞻性、NHLBI 赞助的 PVDOMICS 网络的 PH 患者接受了密集的临床、生物标志物、影像学、气体交换和运动表型分析。在多个表型领域比较了单纯 G2、单纯 G3 或重叠 G2-3 PH 患者。在所有主要为 G2 的患者中(n=136),66 名(49%)被认为有继发性肺部疾病/低氧血症的贡献者(G2/3),在所有被归类为主要 G3 的患者中(n=172),41 名(24%)被判断有继发性 LHD 成分(G3/2),因此有 107 名患者有 G2-3(合并 G2/3 和 G3/2)。与 G3 相比,G2 和 G2-3 患者更肥胖,高血压、心房颤动和冠心病的患病率更高。G2 和 G2-3 患者贫血更严重,肾功能更差,心脏功能障碍更严重,N 末端脑钠肽前体水平更高。G3 和 G2-3 的肺弥散功能均受损,但即使在 G2 中也常异常。所有组的运动能力均严重受损且相似,6 分钟步行距离或峰值耗氧量无差异,一氧化氮诱导的肺血管反应性也无差异。在多变量 Cox 回归模型中,G2 患者的死亡或移植风险低于 G3(风险比[HR]0.51,95%置信区间[CI]0.30-0.86),G2-3 患者的风险也低于 G3(HR 0.57,95% CI 0.38-0.86)。
PH 患者中肺部或心脏基础的重叠很常见。虽然 G3 和 G2-3 的肺结构/功能明显比 G2 受损更严重,但 G2 中也常存在肺部异常,即使临床上判断为孤立性 LHD。需要进一步研究以确定最佳系统评估方法,为合并心肺疾病相关的 PH 指导治疗创新提供指导。
ClinicalTrials.gov NCT02980887。