Medical School of Chinese PLA, Beijing, China.
Medical Big Data Research Center, Chinese PLA General Hospital, Beijing, China.
BMC Geriatr. 2024 Jun 20;24(1):534. doi: 10.1186/s12877-024-04971-w.
Upper gastrointestinal bleeding (UGIB) in older patients is associated with substantial in-hospital morbidity and mortality. This study aimed to develop and validate a simplified risk score for predicting 30-day in-hospital mortality in this population.
A retrospective analysis was conducted on data from 1899 UGIB patients aged ≥ 65 years admitted to a single medical center between January 2010 and December 2019. An additional cohort of 330 patients admitted from January 2020 to October 2021 was used for external validation. Variable selection was performed using five distinct methods, and models were generated using generalized linear models, random forest, support vector machine, and k-nearest neighbors approaches. The developed score, "ABCAP," incorporated Albumin < 30 g/L, Blood Urea Nitrogen (BUN) > 7.5 mmol/L, Cancer presence, Altered mental status, and Pulse rate > 100/min, each assigned a score of 1. Internal and external validation procedures compared the ABCAP score with the AIMS65 score.
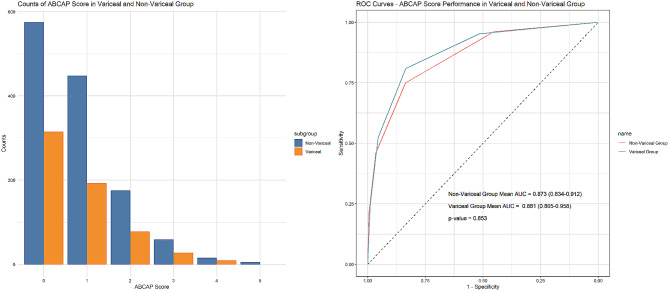
In internal validation, the ABCAP score demonstrated robust predictive capability with an area under the curve (AUC) of 0.878 (95% CI: 0.824-0.932), which was significantly better than the AIMS65 score (AUC: 0.827, 95% CI: 0.751-0.904), as revealed by the DeLong test (p = 0.048). External validation of the ABCAP score resulted in an AUC of 0.799 (95% CI: 0.709-0.889), while the AIMS65 score yielded an AUC of 0.743 (95% CI: 0.647-0.838), with no significant difference between the two scores based on the DeLong test (p = 0.16). However, the ABCAP score at the 3-5 score level demonstrated superior performance in identifying high-risk patients compared to the AIMS65 score. This score exhibited consistent predictive accuracy across variceal and non-variceal UGIB subgroups.
The ABCAP score incorporates easily obtained clinical variables and demonstrates promising predictive ability for 30-day in-hospital mortality in older UGIB patients. It allows effective mortality risk stratification and showed slightly better performance than the AIMS65 score. Further cohort validation is required to confirm generalizability.
老年人上消化道出血(UGIB)与大量院内发病率和死亡率相关。本研究旨在为该人群开发和验证一种简化的风险评分,以预测 30 天院内死亡率。
对 2010 年 1 月至 2019 年 12 月期间在一家医疗中心就诊的 1899 例年龄≥65 岁的 UGIB 患者的数据进行回顾性分析。另外一个队列由 2020 年 1 月至 2021 年 10 月入院的 330 例患者组成,用于外部验证。使用五种不同的方法进行变量选择,并使用广义线性模型、随机森林、支持向量机和 k-最近邻方法生成模型。开发的评分“ABCAP”纳入了白蛋白<30 g/L、血尿素氮(BUN)>7.5 mmol/L、癌症存在、意识状态改变和脉搏率>100/min,每个评分 1 分。内部和外部验证程序将 ABCAP 评分与 AIMS65 评分进行比较。
内部验证中,ABCAP 评分具有稳健的预测能力,曲线下面积(AUC)为 0.878(95%CI:0.824-0.932),明显优于 AIMS65 评分(AUC:0.827,95%CI:0.751-0.904),DeLong 检验显示差异有统计学意义(p=0.048)。ABCAP 评分的外部验证得到 AUC 为 0.799(95%CI:0.709-0.889),而 AIMS65 评分的 AUC 为 0.743(95%CI:0.647-0.838),DeLong 检验显示差异无统计学意义(p=0.16)。然而,在识别高危患者方面,ABCAP 评分在 3-5 分水平上的表现优于 AIMS65 评分。该评分在静脉曲张性和非静脉曲张性 UGIB 亚组中具有一致的预测准确性。
ABCAP 评分纳入了易于获得的临床变量,对老年 UGIB 患者 30 天院内死亡率具有良好的预测能力。它可以有效地进行死亡率风险分层,表现略优于 AIMS65 评分。需要进一步的队列验证来确认其普遍性。