Qiu Weizhi, Liu Chubin, Ye Jinfu, Wang Gang, Yang Fuxing, Pan Zhigang, Hu Weipeng, Gao Hongzhi
Department of Neurosurgery, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, China.
Department of Neurosurgery, The Second Affiliated Clinical Medical College of Fujian Medical University, Quanzhou, China.
Front Neurol. 2023 Feb 13;14:1034865. doi: 10.3389/fneur.2023.1034865. eCollection 2023.
Recent clinical studies have demonstrated that advanced age and low initial Glasgow Coma Scale (GCS) score were independent predictors of gastrointestinal bleeding (GIB) in patients with primary intracerebral hemorrhage (ICH). However, used singly, age and GCS score have their respective shortcomings in predicting the occurrence of GIB. This study aimed to investigate the association between the age-to-initial GCS score ratio (AGR) and the risk of GIB following ICH.
We conducted a single-center, retrospective observational study of consecutive patients presenting with spontaneous primary ICH at our hospital from January 2017 through January 2021. Patients who fulfilled the inclusion and exclusion criteria were categorized into GIB and non-GIB groups. Univariate and multivariate logistic regression analyses were implemented to identify the independent risk factors for the occurrence of GIB, and a multicollinearity test was performed. Furthermore, one-to-one matching was conducted to balance important patient characteristics by the groups' propensity score matching (PSM) analysis.
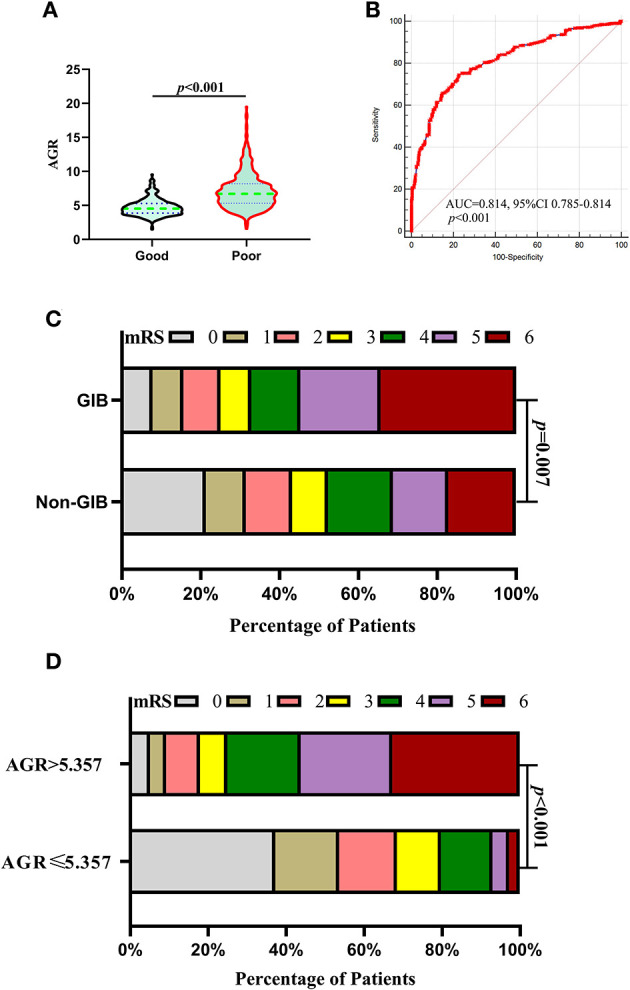
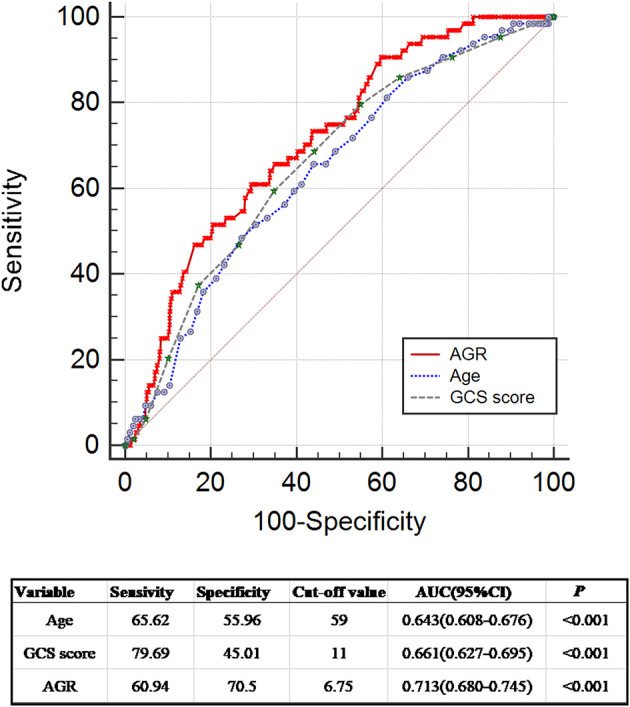
A total of 786 consecutive patients fulfilled the inclusion/exclusion criteria for the study, and 64 (8.14%) patients experienced GIB after primary ICH. Univariate analysis revealed that patients with GIB were significantly older [64.0 (55.0-71.75) years vs. 57.0 (51.0-66.0) years, = 0.001] and had a higher AGR [7.32 (5.24-8.96) vs. 5.40 (4.31-7.11), < 0.001] and a lower initial GCS score [9.0 (7.0-11.0) vs. 11.0 (8.0-13.0) < 0.001]. The multicollinearity test revealed that no multicollinearity was observed in the multivariable models. Multivariate analysis showed that the AGR was a significant independent predictor of GIB [odds ratio (OR) 1.155, 95% confidence interval (CI) 1.041-1.281, = 0.007], as well as prior anticoagulation or antiplatelet therapy (OR 0.388, 95% CI 0.160-0.940, = 0.036) and MV used >24 h (OR 0.462, 95% CI 0.252-0.848, = 0.013). Receiver operating curve (ROC) analysis illustrated that the optimal cutoff value for the AGR as a predictor for GIB in patients with primary ICH was 6.759 [the area under the curve (AUC) was 0.713 with a corresponding sensitivity of 60.94% and specificity of 70.5%, 95% CI 0.680-0.745, < 0.001]. After 1:1 PSM, the matched GIB group had significantly higher AGR levels compared with the matched non-GIB group [7.47(5.38-9.32) vs. 5.24(4.24-6.40), <0.001]. The ROC analysis indicated an AUC of 0.747 (the sensitivity was 65.62%, and the specificity was 75.0%, 95% CI 0.662-0.819, < 0.001) for AGR levels as an independent predictor of GIB in patients with ICH. In addition, AGR levels were statistically correlated with unfunctional 90-day outcomes.
A higher AGR was associated with an increased risk of GIB and unfunctional 90-day outcomes in patients with primary ICH.
近期临床研究表明,高龄和初始格拉斯哥昏迷量表(GCS)评分低是原发性脑出血(ICH)患者发生胃肠道出血(GIB)的独立预测因素。然而,单独使用年龄和GCS评分在预测GIB发生方面各自存在缺陷。本研究旨在探讨年龄与初始GCS评分比值(AGR)与ICH后发生GIB风险之间的关联。
我们对2017年1月至2021年1月在我院连续就诊的自发性原发性ICH患者进行了单中心回顾性观察研究。符合纳入和排除标准的患者被分为GIB组和非GIB组。进行单因素和多因素逻辑回归分析以确定GIB发生的独立危险因素,并进行了多重共线性检验。此外,通过两组的倾向得分匹配(PSM)分析进行一对一匹配以平衡重要的患者特征。
共有786例连续患者符合研究的纳入/排除标准,其中64例(8.14%)患者在原发性ICH后发生了GIB。单因素分析显示,GIB患者年龄显著更大[64.0(55.0 - 71.75)岁 vs. 57.0(51.0 - 66.0)岁,P = 0.001],AGR更高[7.32(5.24 - 8.96) vs. 5.40(4.31 - 7.11),P < 0.001],初始GCS评分更低[9.0(7.0 - 11.0) vs. 11.0(8.0 - 13.0),P < 0.001]。多重共线性检验显示多变量模型中未观察到多重共线性。多因素分析表明,AGR是GIB的显著独立预测因素[比值比(OR)1.155,95%置信区间(CI)1.041 - 1.281,P = 0.007],以及既往抗凝或抗血小板治疗(OR 0.388,95% CI 0.160 - 0.940,P = 0.036)和机械通气(MV)使用>24小时(OR 0.462,95% CI 0.252 - 0.848,P = 0.013)。受试者工作特征曲线(ROC)分析表明,原发性ICH患者中AGR作为GIB预测指标的最佳截断值为6.759[曲线下面积(AUC)为0.713,相应的灵敏度为60.94%,特异度为70.5%,95% CI 0.680 - 0.745,P < 0.001]。经过1:1 PSM后,匹配的GIB组AGR水平显著高于匹配的非GIB组[7.47(5.38 - 9.32) vs. 5.24(4.24 - 6.40),P < 0.001]。ROC分析表明,AGR水平作为ICH患者GIB独立预测指标的AUC为0.747(灵敏度为65.62%,特异度为75.0%,95% CI 0.662 - 0.819,P < 0.001)。此外,AGR水平与90天无功能结局在统计学上相关。
较高的AGR与原发性ICH患者发生GIB的风险增加及90天无功能结局相关。