Department of Clinical Pharmacology, Medical University of Vienna, Waehringer Guertel 18-20, 1090, Vienna, Austria.
Department of Medicine, Pulmonary Sciences and Critical Care, Anschutz Medical Campus, Denver Health and University of Colorado, Denver, CO, USA.
Crit Care. 2024 Jul 11;28(1):231. doi: 10.1186/s13054-024-05019-6.
Early fluid management in patients with advanced chronic kidney disease (CKD) and sepsis-induced hypotension is challenging with limited evidence to support treatment recommendations. We aimed to compare an early restrictive versus liberal fluid management for sepsis-induced hypotension in patients with advanced CKD.
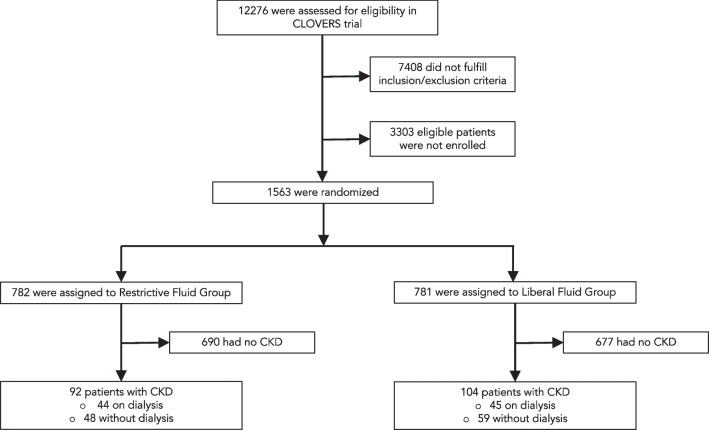
This post-hoc analysis included patients with advanced CKD (eGFR of less than 30 mL/min/1.73 m or history of end-stage renal disease on chronic dialysis) from the crystalloid liberal or vasopressor early resuscitation in sepsis (CLOVERS) trial. The primary endpoint was death from any cause before discharge home by day 90.
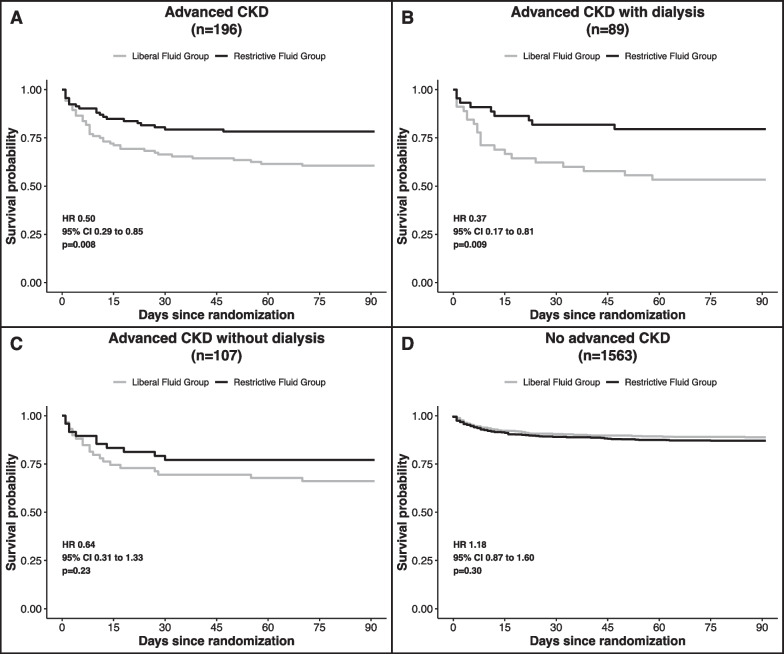
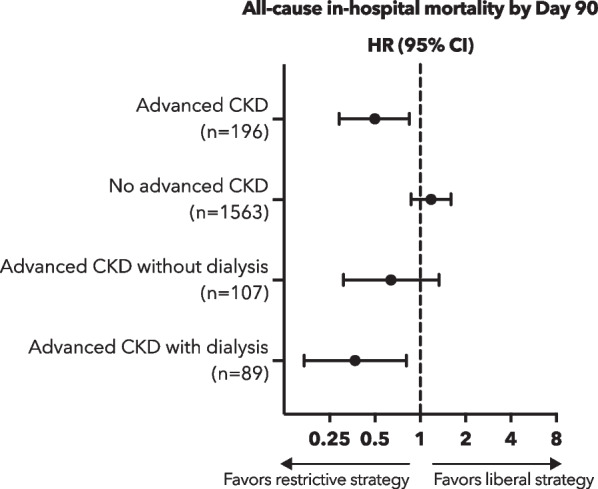
Of 1563 participants enrolled in the CLOVERS trial, 196 participants had advanced CKD (45% on chronic dialysis), with 92 participants randomly assigned to the restrictive treatment group and 104 assigned to the liberal fluid group. Death from any cause before discharge home by day 90 occurred significantly less often in the restrictive fluid group compared with the liberal fluid group (20 [21.7%] vs. 41 [39.4%], HR 0.5, 95% CI 0.29-0.85). Participants in the restrictive fluid group had more vasopressor-free days (19.7 ± 10.4 days vs. 15.4 ± 12.6 days; mean difference 4.3 days, 95% CI, 1.0-7.5) and ventilator-free days by day 28 (21.0 ± 11.8 vs. 16.5 ± 13.6 days; mean difference 4.5 days, 95% CI, 0.9-8.1).
In patients with advanced CKD and sepsis-induced hypotension, an early restrictive fluid strategy, prioritizing vasopressor use, was associated with a lower risk of death from any cause before discharge home by day 90 as compared with an early liberal fluid strategy.
NCT03434028 (2018-02-09), BioLINCC 14149.
对于合并晚期慢性肾脏病(CKD)和脓毒症性低血压的患者,早期液体管理颇具挑战,目前仅有有限的证据支持治疗推荐。本研究旨在比较早期限制性与开放性液体管理策略对合并晚期 CKD 患者脓毒性低血压的疗效。
本研究为事后分析,纳入了来自晶体液开放性或升压药早期复苏治疗脓毒症(CLOVERS)试验的合并晚期 CKD(估算肾小球滤过率[eGFR]<30 mL/min/1.73 m 或既往慢性透析的终末期肾病)患者。主要终点为 90 天内出院回家前的任何原因死亡率。
CLOVERS 试验共纳入了 1563 名患者,其中 196 名患者合并晚期 CKD(45%接受慢性透析),其中 92 名患者被随机分配至限制性液体治疗组,104 名患者被分配至开放性液体组。与开放性液体组相比,限制性液体组出院回家前的任何原因死亡率显著降低(20 [21.7%] vs. 41 [39.4%],HR 0.5,95% CI 0.29-0.85)。与开放性液体组相比,限制性液体组患者的无升压药天数(19.7±10.4 天 vs. 15.4±12.6 天;平均差异 4.3 天,95% CI,1.0-7.5)和 28 天的无呼吸机天数(21.0±11.8 天 vs. 16.5±13.6 天;平均差异 4.5 天,95% CI,0.9-8.1)均更长。
对于合并晚期 CKD 和脓毒症性低血压的患者,与早期开放性液体策略相比,早期优先使用升压药的限制性液体策略可降低 90 天内出院回家前任何原因死亡率。
NCT03434028(2018-02-09),BioLINCC 14149。