Centre for Advancing Health Outcomes, St. Paul's Hospital, Vancouver, British Columbia, Canada.
Faculty of Health Sciences, Simon Fraser University, Burnaby, British Columbia, Canada.
J Int AIDS Soc. 2024 Jul;27(7):e26322. doi: 10.1002/jia2.26322.
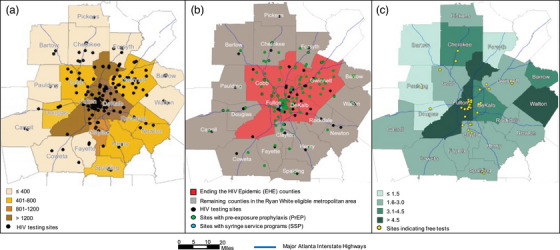
Four counties within the Atlanta, Georgia 20-county eligible metropolitan area (EMA) are currently prioritized by the US "Ending the HIV Epidemic" (EHE) initiative which aims for a 90% reduction in HIV incidence by 2030. Disparities driving Atlanta's HIV epidemic warrant an examination of local service availability, unmet needs and organizational capacity to reach EHE targets. We conducted a mixed-methods evaluation of the Atlanta EMA to examine geographic HIV epidemiology and distribution of services, service needs and organization infrastructure for each pillar of the EHE initiative.
We collected 2021 county-level data (during June 2022), from multiple sources including: AIDSVu (HIV prevalence and new diagnoses), the Centers for Disease Control and Prevention web-based tools (HIV testing and pre-exposure prophylaxis [PrEP] locations) and the Georgia Department of Public Health (HIV testing, PrEP screenings, viral suppression and partner service interviews). We additionally distributed an online survey to key local stakeholders working at major HIV care agencies across the EMA to assess the availability of services, unmet needs and organization infrastructure (June-December 2022). The Organizational Readiness for Implementing Change questionnaire assessed the organization climate for services in need of scale-up or implementation.
We found racial/ethnic and geographic disparities in HIV disease burden and service availability across the EMA-particularly for HIV testing and PrEP in the EMA's southern counties. Five counties not currently prioritized by EHE (Clayton, Douglas, Henry, Newton and Rockdale) accounted for 16% of the EMA's new diagnoses, but <9% of its 177 testing sites and <7% of its 130 PrEP sites. Survey respondents (N = 48; 42% health agency managers/directors) reported high unmet need for HIV self-testing kits, mobile clinic testing, HIV case management, peer outreach and navigation, integrated care, housing support and transportation services. Respondents highlighted insufficient existing staffing and infrastructure to facilitate the necessary expansion of services, and the need to reduce inequities and address intersectional stigma.
Service delivery across all EHE pillars must substantially expand to reach national goals and address HIV disparities in metro Atlanta. High-resolution geographic data on HIV epidemiology and service delivery with community input can provide targeted guidance to support local EHE efforts.
美国“终结艾滋疫情”(EHE)倡议目前将佐治亚州亚特兰大市 20 个县合格大都市区(EMA)内的四个县列为优先重点,该倡议旨在到 2030 年将艾滋病毒发病率降低 90%。推动亚特兰大艾滋病毒疫情的差异需要对当地服务的可及性、未满足的需求以及实现 EHE 目标的组织能力进行审查。我们对亚特兰大 EMA 进行了混合方法评估,以检查艾滋病毒的地理流行病学和服务分布,以及 EHE 倡议每一个支柱的服务需求和组织基础设施。
我们收集了 2021 年县级数据(2022 年 6 月),来源包括:AIDSVu(艾滋病毒流行率和新诊断)、疾病控制与预防中心网络工具(艾滋病毒检测和暴露前预防 [PrEP] 地点)和佐治亚州公共卫生部(艾滋病毒检测、PrEP 筛查、病毒抑制和伙伴服务访谈)。我们还向 EMA 内主要艾滋病毒护理机构的主要利益相关者分发了在线调查,以评估服务的可及性、未满足的需求和组织基础设施(2022 年 6 月至 12 月)。组织变革实施准备情况调查问卷评估了需要扩大规模或实施的服务的组织氛围。
我们发现 EMA 内艾滋病毒疾病负担和服务提供存在种族/族裔和地理差异-特别是在 EMA 南部各县的艾滋病毒检测和 PrEP 方面。五个目前未被 EHE 优先考虑的县(克莱顿、道格拉斯、亨利、牛顿和罗克代尔)占 EMA 新诊断的 16%,但只有不到 9%的检测点和不到 7%的 PrEP 点。调查受访者(N = 48;42%为卫生机构管理人员/主任)报告说,艾滋病毒自我检测包、移动诊所检测、艾滋病毒病例管理、同伴外展和导航、综合护理、住房支持和交通服务方面存在高度未满足的需求。受访者强调现有的人员配置和基础设施不足以促进服务的必要扩展,需要减少不平等现象和解决交叉性耻辱问题。
必须大幅扩大所有 EHE 支柱的服务提供,以实现国家目标并解决亚特兰大大都市的艾滋病毒差异。具有社区投入的艾滋病毒流行病学和服务提供的高分辨率地理数据可以为支持当地 EHE 工作提供有针对性的指导。