Cuomo Gianluigi, Di Lorenzo Anna, Tramontano Anna, Iannone Francesca Paola, D'Angelo Andrea, Pezzella Rita, Testa Crescenzo, Parlato Alessandro, Merone Pasquale, Pacileo Mario, D'Andrea Antonello, Cudemo Giuseppe, Venturini Elio, Iannuzzo Gabriella, Vigorito Carlo, Giallauria Francesco
Department of Translational Medical Sciences, "Federico II" University of Naples, 80131 Naples, Italy.
Division of Cardiology/UTIC, "Umberto I" Hospital, Nocera Inferiore (ASL Salerno), 84014 Nocera Inferiore (SA), Italy.
Rev Cardiovasc Med. 2022 Apr 12;23(4):144. doi: 10.31083/j.rcm2304144. eCollection 2022 Apr.
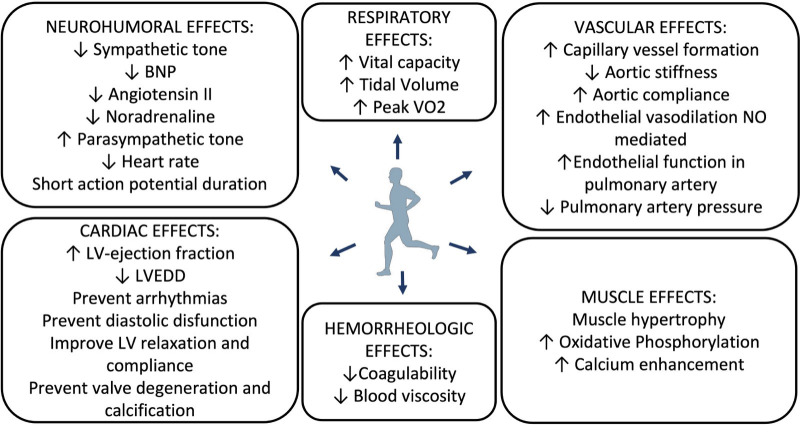
Heart failure (HF) is a chronic, progressive, and inexorable syndrome affecting worldwide billion of patients (equally distributed among men and women), with prevalence estimate of 1-3% in developed countries. HF leads to enormous direct and indirect costs, and because of ageing population, the total number of HF patients keep rising, approximately 10% in patients 65 years old. Exercise training (ET) is widely recognized as an evidence-based adjunct treatment modality for patients with HF, and growing evidence is emerging among elderly patients with HF. We used relevant data from literature search (PubMed, Medline, EMBASE) highlighting the epidemiology of HF; focusing on central and peripheral mechanisms underlying the beneficial effect of ET in HF patients; and on frail HF elderly patients undergoing ET. Since many Countries ordered a lockdown in early stages pandemic trying to limit infections, COVID-19 pandemic, and its limitation to exercise-based cardiac rehabilitation operativity was also discussed. ET exerts both central and peripheral adaptations that clinically translate into anti-remodeling effects, increased functional capacity and reduced morbidity and mortality. Ideally, ET programs should be prescribed in a patient-tailored approach, particularly in frail elderly patients with HF. In conclusion, given the complexity of HF syndrome, combining, and tailoring different ET modalities is mandatory. A procedural algorithm according to patient's baseline clinical characteristics [i.e., functional capacity, comorbidity, frailty status (muscle strength, balance, usual daily activities, hearing and vision impairment, sarcopenia, and inability to actively exercise), logistics, individual preferences and goals] has been proposed. Increasing long-term adherence and reaching the frailest patients are challenging goals for future initiatives in the field.
心力衰竭(HF)是一种慢性、进行性且不可避免的综合征,影响着全球数十亿患者(男女分布均衡),在发达国家的患病率估计为1%至3%。HF导致了巨大的直接和间接成本,并且由于人口老龄化,HF患者的总数持续上升,65岁患者中约有10%患病。运动训练(ET)被广泛认为是HF患者基于证据的辅助治疗方式,并且在老年HF患者中的证据越来越多。我们使用了文献检索(PubMed、Medline、EMBASE)中的相关数据,重点关注HF的流行病学;ET对HF患者有益作用的中枢和外周机制;以及接受ET的体弱HF老年患者。由于许多国家在疫情早期下令封锁以试图限制感染,因此还讨论了2019冠状病毒病疫情及其对基于运动的心脏康复可操作性的限制。ET会产生中枢和外周适应性变化,在临床上转化为抗重塑作用、增加功能能力以及降低发病率和死亡率。理想情况下,ET计划应以患者个体化的方式制定,尤其是对于体弱的老年HF患者。总之,鉴于HF综合征的复杂性,必须结合并定制不同的ET方式。已提出一种根据患者基线临床特征[即功能能力、合并症、体弱状态(肌肉力量、平衡、日常活动、听力和视力损害、肌肉减少症以及无法主动运动)、后勤、个人偏好和目标]的程序算法。提高长期依从性并惠及最体弱的患者是该领域未来举措面临的具有挑战性的目标。