The Walter and Eliza Hall Institute of Medical Research, Parkville, VIC, Australia.
Department of Medical Biology, University of Melbourne, Parkville, VIC, Australia.
Mol Cancer. 2024 Aug 5;23(1):158. doi: 10.1186/s12943-024-02048-1.
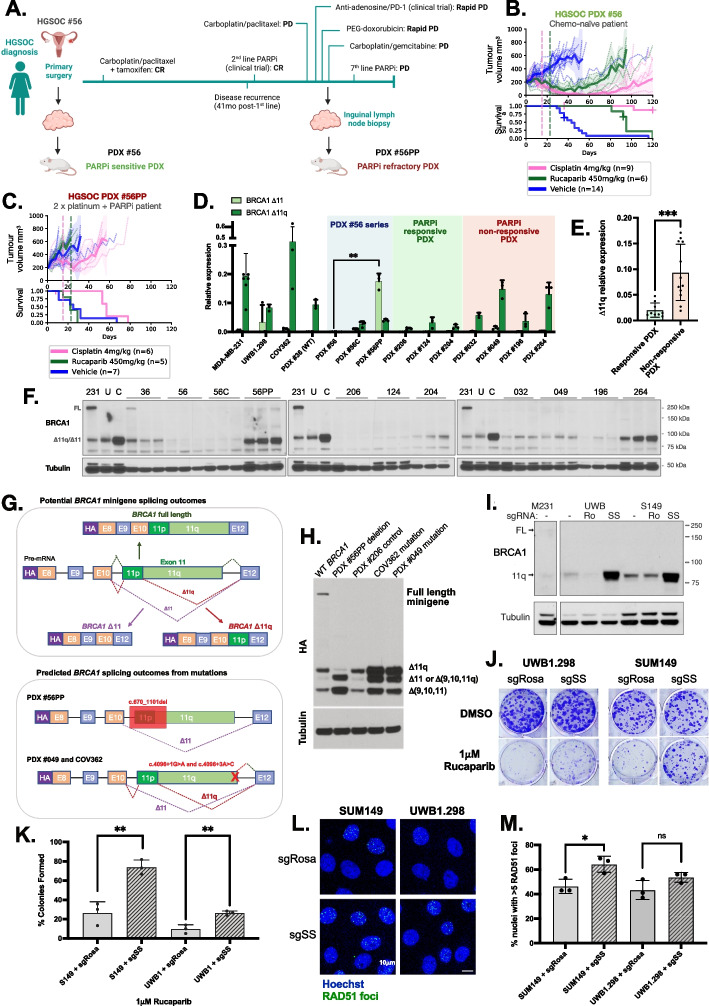
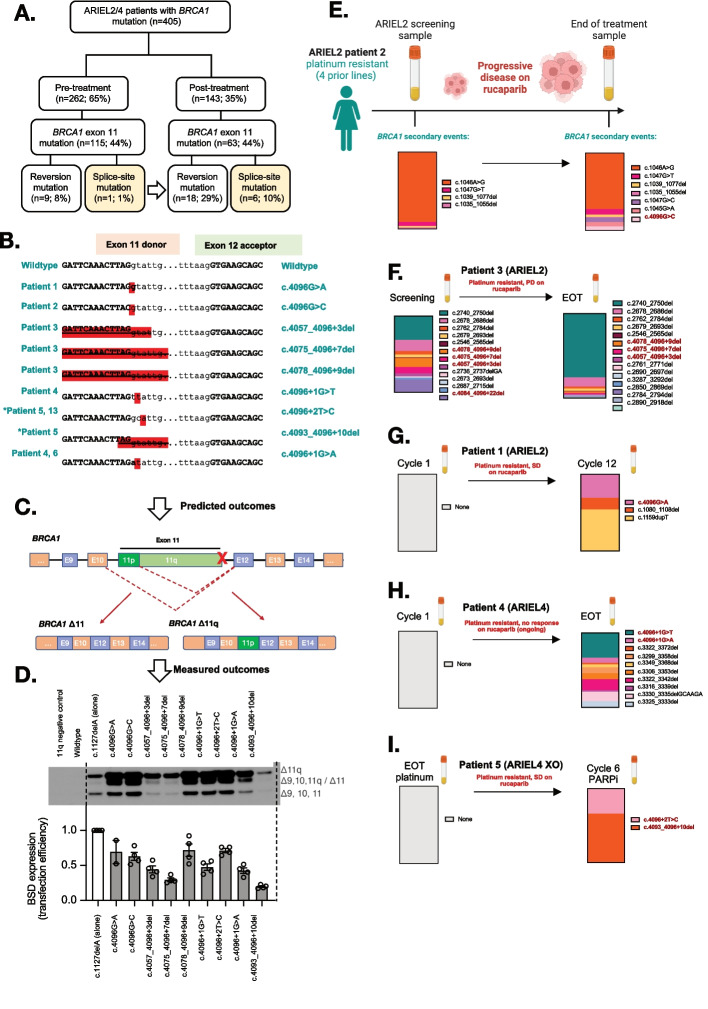
PARP inhibitor (PARPi) therapy has transformed outcomes for patients with homologous recombination DNA repair (HRR) deficient ovarian cancers, for example those with BRCA1 or BRCA2 gene defects. Unfortunately, PARPi resistance is common. Multiple resistance mechanisms have been described, including secondary mutations that restore the HR gene reading frame. BRCA1 splice isoforms △11 and △11q can contribute to PARPi resistance by splicing out the mutation-containing exon, producing truncated, partially functional proteins. However, the clinical impacts and underlying drivers of BRCA1 exon skipping are not fully understood.We analyzed nine ovarian and breast cancer patient derived xenografts (PDX) with BRCA1 exon 11 frameshift mutations for exon skipping and therapy response, including a matched PDX pair derived from a patient pre- and post-chemotherapy/PARPi. BRCA1 exon 11 skipping was elevated in PARPi resistant PDX tumors. Two independent PDX models acquired secondary BRCA1 splice site mutations (SSMs) that drive exon skipping, confirmed using qRT-PCR, RNA sequencing, immunoblotting and minigene modelling. CRISPR/Cas9-mediated disruption of splicing functionally validated exon skipping as a mechanism of PARPi resistance. SSMs were also enriched in post-PARPi ovarian cancer patient cohorts from the ARIEL2 and ARIEL4 clinical trials.Few PARPi resistance mechanisms have been confirmed in the clinical setting. While secondary/reversion mutations typically restore a gene's reading frame, we have identified secondary mutations in patient cohorts that hijack splice sites to enhance mutation-containing exon skipping, resulting in the overexpression of BRCA1 hypomorphs, which in turn promote PARPi resistance. Thus, BRCA1 SSMs can and should be clinically monitored, along with frame-restoring secondary mutations.
聚腺苷二磷酸核糖聚合酶(PARP)抑制剂(PARPi)治疗改变了同源重组 DNA 修复(HRR)缺陷的卵巢癌患者的预后,例如 BRCA1 或 BRCA2 基因突变的患者。不幸的是,PARPi 耐药很常见。已经描述了多种耐药机制,包括恢复 HR 基因阅读框的继发突变。BRCA1 剪接异构体 △11 和 △11q 可以通过剪接出含有突变的外显子,产生截断的、部分功能的蛋白质,从而导致 PARPi 耐药。然而,BRCA1 外显子跳跃的临床影响和潜在驱动因素尚未完全了解。我们分析了 9 例具有 BRCA1 外显子 11 移码突变的卵巢癌和乳腺癌患者来源异种移植(PDX)的外显子跳跃和治疗反应,包括一对来自化疗/ PARPi 前后患者的匹配 PDX 对。PARPi 耐药的 PDX 肿瘤中 BRCA1 外显子 11 跳跃增加。两个独立的 PDX 模型获得了驱动外显子跳跃的二次 BRCA1 剪接位点突变(SSM),通过 qRT-PCR、RNA 测序、免疫印迹和小基因建模得到证实。CRISPR/Cas9 介导的剪接中断功能验证了外显子跳跃作为 PARPi 耐药的机制。SSM 也在 ARIEL2 和 ARIEL4 临床试验的卵巢癌患者队列中富集。在临床环境中已经证实了几种 PARPi 耐药机制。虽然继发/回复突变通常会恢复基因的阅读框,但我们在患者队列中发现了二次突变,这些突变劫持剪接位点以增强含有突变的外显子跳跃,从而导致 BRCA1 低等位基因的过表达,进而促进 PARPi 耐药。因此,BRCA1 SSM 可以而且应该与恢复框架的继发突变一起进行临床监测。