Experimental Therapeutics Group; High Risk and Familial Cancer, Vall d'Hebron Institute of Oncology, Barcelona; Department of Medical Oncology, Hospital Vall d'Hebron, Universitat Autònoma de Barcelona, Barcelona.
Experimental Therapeutics Group.
Ann Oncol. 2018 May 1;29(5):1203-1210. doi: 10.1093/annonc/mdy099.
BRCA1 and BRCA2 (BRCA1/2)-deficient tumors display impaired homologous recombination repair (HRR) and enhanced sensitivity to DNA damaging agents or to poly(ADP-ribose) polymerase (PARP) inhibitors (PARPi). Their efficacy in germline BRCA1/2 (gBRCA1/2)-mutated metastatic breast cancers has been recently confirmed in clinical trials. Numerous mechanisms of PARPi resistance have been described, whose clinical relevance in gBRCA-mutated breast cancer is unknown. This highlights the need to identify functional biomarkers to better predict PARPi sensitivity.
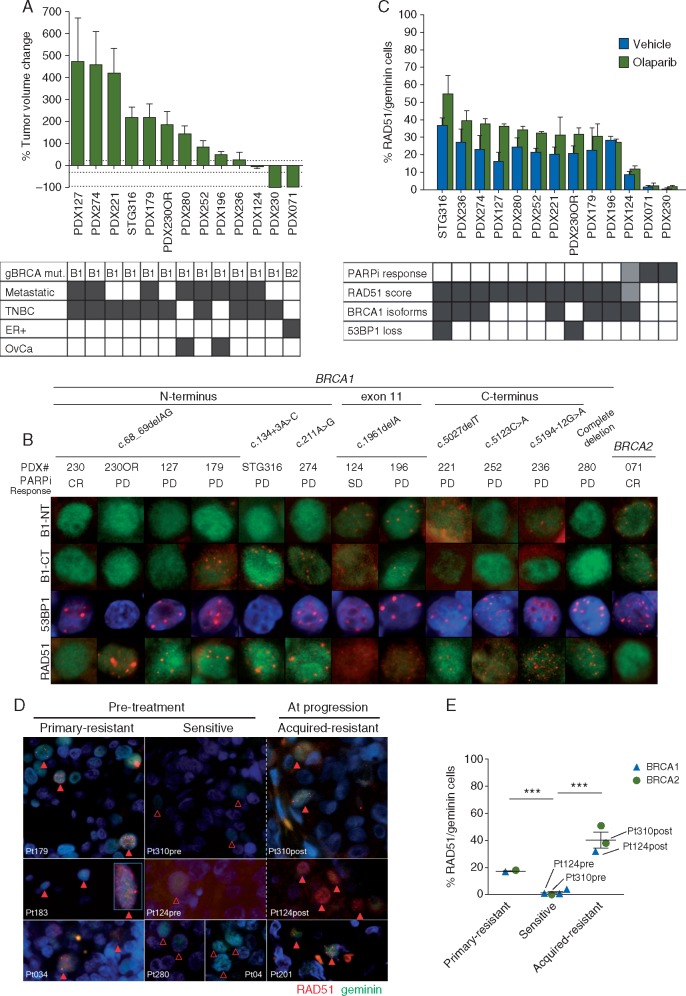
We investigated the in vivo mechanisms of PARPi resistance in gBRCA1 patient-derived tumor xenografts (PDXs) exhibiting differential response to PARPi. Analysis included exome sequencing and immunostaining of DNA damage response proteins to functionally evaluate HRR. Findings were validated in a retrospective sample set from gBRCA1/2-cancer patients treated with PARPi.
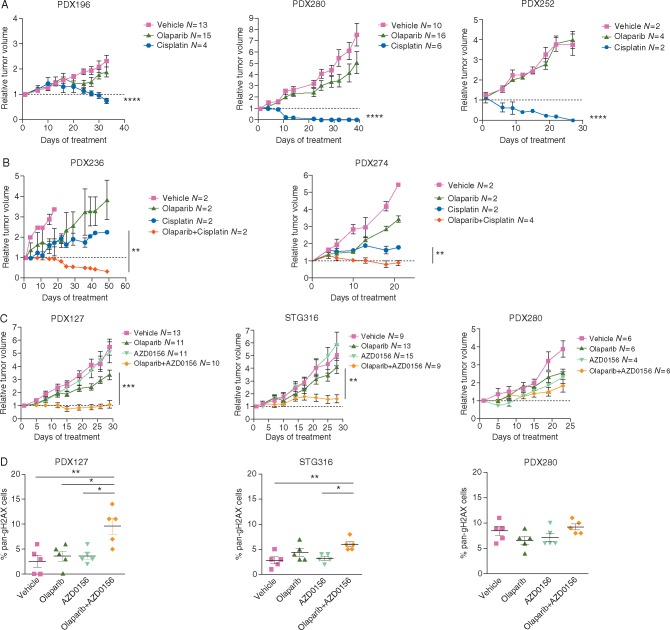
RAD51 nuclear foci, a surrogate marker of HRR functionality, were the only common feature in PDX and patient samples with primary or acquired PARPi resistance. Consistently, low RAD51 was associated with objective response to PARPi. Evaluation of the RAD51 biomarker in untreated tumors was feasible due to endogenous DNA damage. In PARPi-resistant gBRCA1 PDXs, genetic analysis found no in-frame secondary mutations, but BRCA1 hypomorphic proteins in 60% of the models, TP53BP1-loss in 20% and RAD51-amplification in one sample, none mutually exclusive. Conversely, one of three PARPi-resistant gBRCA2 tumors displayed BRCA2 restoration by exome sequencing. In PDXs, PARPi resistance could be reverted upon combination of a PARPi with an ataxia-telangiectasia mutated (ATM) inhibitor.
Detection of RAD51 foci in gBRCA tumors correlates with PARPi resistance regardless of the underlying mechanism restoring HRR function. This is a promising biomarker to be used in the clinic to better select patients for PARPi therapy. Our study also supports the clinical development of PARPi combinations such as those with ATM inhibitors.
BRCA1 和 BRCA2(BRCA1/2)缺陷型肿瘤表现出同源重组修复(HRR)受损和对 DNA 损伤剂或聚(ADP-核糖)聚合酶(PARP)抑制剂(PARPi)的敏感性增强。最近在临床试验中证实了它们在种系 BRCA1/2(gBRCA1/2)突变转移性乳腺癌中的疗效。已经描述了许多 PARPi 耐药机制,但其在 gBRCA 突变乳腺癌中的临床相关性尚不清楚。这凸显了需要识别功能生物标志物以更好地预测 PARPi 敏感性的必要性。
我们研究了在对 PARPi 表现出不同反应的 gBRCA1 患者来源肿瘤异种移植物(PDX)中 PARPi 耐药的体内机制。分析包括外显子组测序和 DNA 损伤反应蛋白的免疫染色,以功能评估 HRR。在接受 PARPi 治疗的 gBRCA1/2 癌症患者的回顾性样本集中验证了这些发现。
RAD51 核焦点,HRR 功能的替代标志物,是 PDX 和患者样本中具有原发性或获得性 PARPi 耐药性的唯一共同特征。一致地,RAD51 低与对 PARPi 的客观反应相关。由于内源性 DNA 损伤,在未治疗的肿瘤中评估 RAD51 生物标志物是可行的。在 PARPi 耐药的 gBRCA1 PDX 中,遗传分析未发现框内二级突变,但在 60%的模型中发现 BRCA1 低功能蛋白,20%的模型中发现 TP53BP1 缺失,1 个样本中发现 RAD51 扩增,但没有相互排斥。相反,三例 PARPi 耐药的 gBRCA2 肿瘤中有一例通过外显子组测序发现 BRCA2 恢复。在 PDX 中,PARPi 耐药性可以通过 PARPi 与共济失调毛细血管扩张突变(ATM)抑制剂联合使用来逆转。
无论 HRR 功能恢复的潜在机制如何,在 gBRCA 肿瘤中检测到 RAD51 焦点与 PARPi 耐药相关。这是一种有前途的生物标志物,可用于临床更好地选择接受 PARPi 治疗的患者。我们的研究还支持 PARPi 联合治疗的临床开发,例如与 ATM 抑制剂的联合治疗。