Sherry Alexander D, Msaouel Pavlos, Kupferman Gabrielle S, Lin Timothy A, Abi Jaoude Joseph, Kouzy Ramez, El-Alam Molly B, Patel Roshal, Koong Alex, Lin Christine, Passy Adina H, Miller Avital M, Beck Esther J, Fuller C David, Meirson Tomer, McCaw Zachary R, Ludmir Ethan B
Department of Radiation Oncology, Division of Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Department of Genitourinary Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
medRxiv. 2024 Jul 24:2024.07.23.24310891. doi: 10.1101/2024.07.23.24310891.
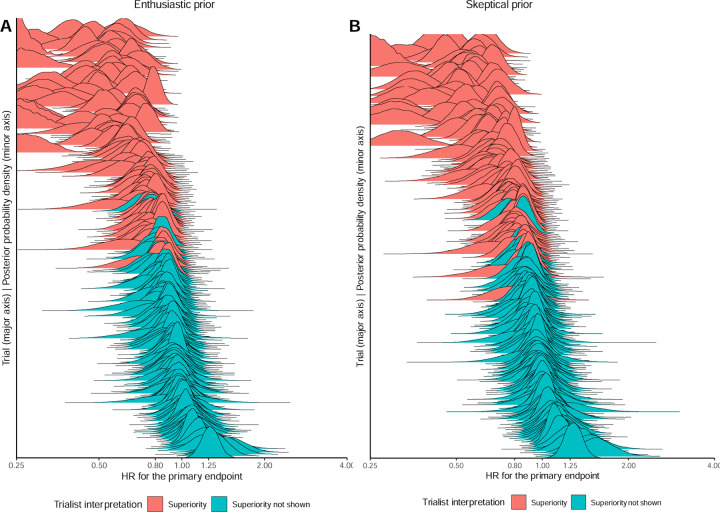
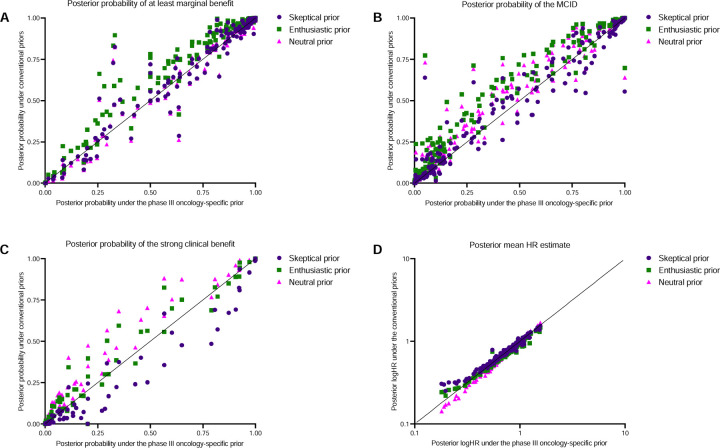
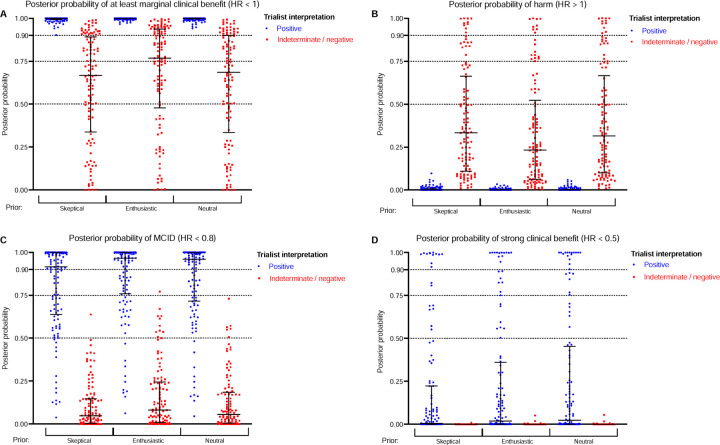
Most oncology trials define superiority of an experimental therapy compared to a control therapy according to frequentist significance thresholds, which are widely misinterpreted. Posterior probability distributions computed by Bayesian inference may be more intuitive measures of uncertainty, particularly for measures of clinical benefit such as the minimum clinically important difference (MCID). Here, we manually reconstructed 194,129 individual patient-level outcomes across 230 phase III, superiority-design, oncology trials. Posteriors were calculated by Markov Chain Monte Carlo sampling using standard priors. All trials interpreted as positive had probabilities > 90% for marginal benefits (HR < 1). However, 38% of positive trials had ≤ 90% probabilities of achieving the MCID (HR < 0.8), even under an enthusiastic prior. A subgroup analysis of 82 trials that led to regulatory approval showed 30% had ≤ 90% probability for meeting the MCID under an enthusiastic prior. Conversely, 24% of negative trials had > 90% probability of achieving marginal benefits, even under a skeptical prior, including 12 trials with a primary endpoint of overall survival. Lastly, a phase III oncology-specific prior from a previous work, which uses published summary statistics rather than reconstructed data to compute posteriors, validated the individual patient-level data findings. Taken together, these results suggest that Bayesian models add considerable unique interpretative value to phase III oncology trials and provide a robust solution for overcoming the discrepancies between refuting the null hypothesis and obtaining a MCID.
大多数肿瘤学试验根据频率主义显著性阈值来定义实验疗法相对于对照疗法的优越性,而这些阈值被广泛误解。通过贝叶斯推理计算出的后验概率分布可能是更直观的不确定性度量,特别是对于临床获益度量,如最小临床重要差异(MCID)。在此,我们手动重建了230项III期、优效性设计的肿瘤学试验中194,129个个体患者水平的结局。后验概率通过使用标准先验的马尔可夫链蒙特卡罗抽样计算得出。所有被解释为阳性的试验,其边际获益(风险比<1)的概率均>90%。然而,38%的阳性试验即使在先验较为乐观的情况下,实现MCID(风险比<0.8)的概率也≤90%。对82项获得监管批准的试验进行的亚组分析显示,在先验较为乐观的情况下,30%的试验达到MCID的概率≤90%。相反,24%的阴性试验即使在先验较为怀疑的情况下,实现边际获益的概率也>90%,其中包括12项以总生存为主要终点的试验。最后,一项先前研究中针对肿瘤学的III期特定先验,它使用已发表的汇总统计数据而非重建数据来计算后验概率,验证了个体患者水平数据的研究结果。综上所述,这些结果表明贝叶斯模型为III期肿瘤学试验增添了相当大的独特解释价值,并为克服反驳原假设与获得MCID之间的差异提供了一个可靠的解决方案。