Payne Rebecca, Dakin Francesca, MacIver Ellen, Swann Nadia, Pring Tabitha, Clarke Aileen, Kalin Asli, Moore Lucy, Ladds Emma, Wherton Joseph, Rybczynska-Bunt Sarah, Husain Laiba, Hemmings Nina, Wieringa Sietse, Greenhalgh Trisha
Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford.
Peninsula Schools of Medicine and Dentistry, University of Plymouth, Plymouth.
Br J Gen Pract. 2024 Dec 26;75(750):e1-e11. doi: 10.3399/BJGP.2024.0184. Print 2025 Jan.
Since 2022, general practice has shifted from responding to the acute challenges of COVID-19 to restoring full services using a hybrid of remote, digital, and in-person care.
To examine how quality domains are addressed in contemporary UK general practice.
Multi-site, mostly qualitative longitudinal case study, placed in UK national policy context.
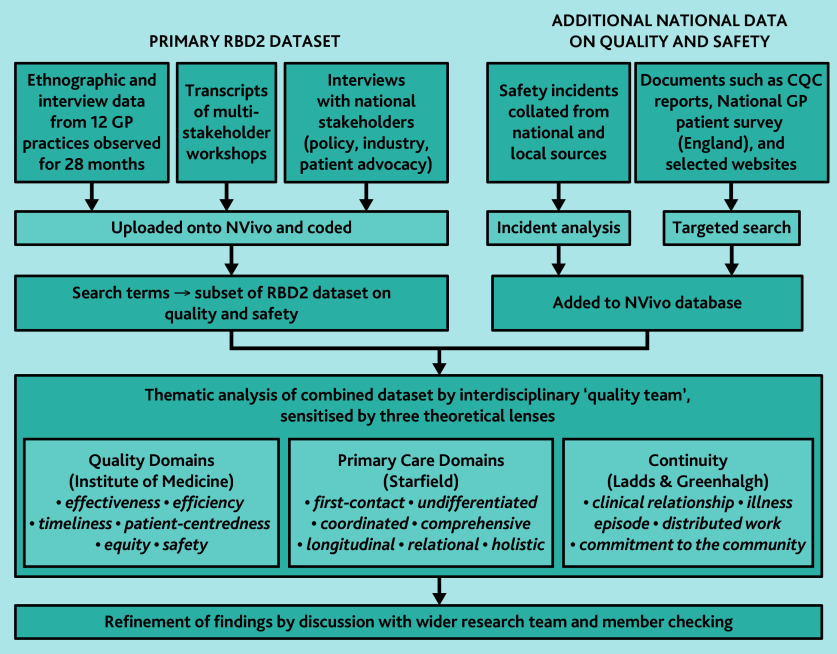
Data were collected from longitudinal ethnographic case studies of 12 general practices (2021-2023), multi-stakeholder workshops, stakeholder interviews, patient surveys, official reports, and publicly accessible patient experience data. Data were coded thematically and analysed using multiple theories of quality.
Quality efforts in UK general practice occur in the context of cumulative impacts of financial austerity, loss of resilience, increasingly complex patterns of illness and need, a diverse and fragmented workforce, material and digital infrastructure that is unfit for purpose, and physically distant and asynchronous ways of working. Providing the human elements of traditional general practice (such as relationship-based care, compassion, and support) is difficult and sometimes even impossible. Systems designed to increase efficiency have introduced new forms of inefficiency and have compromised other quality domains such as accessibility, patient-centredness, and equity. Long-term condition management varies in quality. Measures to mitigate digital exclusion (such as digital navigators) are welcome but do not compensate for extremes of structural disadvantage. Many staff are stressed and demoralised.
Contemporary hybrid general practice features changes (digitalisation, physical distancing, extension of roles, and protocolisation) that have had the unintended effect of dehumanising, compromising, and fragmenting care. Policymakers and practices should urgently address the risks to patients and the traditional core values of general practice should be urgently addressed.
自2022年以来,全科医疗已从应对新冠疫情的急性挑战转向采用远程、数字和面对面护理相结合的方式恢复全面服务。
探讨当代英国全科医疗中质量领域是如何得到处理的。
多地点、主要为定性的纵向案例研究,置于英国国家政策背景下。
数据收集自12家全科诊所的纵向人种志案例研究(2021 - 2023年)、多利益相关方研讨会、利益相关方访谈、患者调查、官方报告以及可公开获取的患者体验数据。数据进行主题编码,并运用多种质量理论进行分析。
英国全科医疗中的质量工作是在财政紧缩的累积影响、恢复力丧失、疾病和需求模式日益复杂、劳动力多样且分散、物质和数字基础设施不适用以及工作地点遥远和异步等背景下开展的。提供传统全科医疗的人文要素(如基于关系的护理、同情心和支持)困难重重,有时甚至无法实现。旨在提高效率的系统引入了新的低效率形式,并损害了其他质量领域,如可及性、以患者为中心和公平性。长期病症管理的质量参差不齐。减轻数字排斥的措施(如数字导航员)值得欢迎,但无法弥补极端的结构性劣势。许多工作人员压力大且士气低落。
当代混合式全科医疗的特点(数字化、物理距离、角色扩展和规范化)产生了意外后果,使护理变得非人性化、受到损害且碎片化。政策制定者和医疗机构应紧急应对对患者的风险,传统全科医疗的核心价值观也应紧急得到重视。