School of Medical Sciences, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia.
Brain and Mind Centre, University of Sydney, Australia.
JAMA Netw Open. 2024 Aug 1;7(8):e2424139. doi: 10.1001/jamanetworkopen.2024.24139.
Chemotherapy-induced peripheral neuropathy (CIPN) is a substantial adverse effect of anticancer treatments. As such, the assessment of CIPN remains critically important in both research and clinic settings.
To compare the validity of various patient-reported outcome measures (PROMs) with neurophysiological and sensory functional measures as the optimal method of CIPN assessment.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study evaluated participants treated with neurotoxic chemotherapy across 2 cohorts using a dual-study design. Participants commencing treatment were assessed prospectively at beginning of neurotoxic treatment, midtreatment, and at the end of treatment. Participants who completed treatment up to 5 years prior were assessed cross-sectionally and completed a single assessment time point. Participants were recruited from oncology centers in Australia from August 2015 to November 2022. Data analysis occurred from February to November 2023.
Neurotoxic cancer treatment including taxanes, platinums, vinca-alkaloids, proteasome inhibitors, and thalidomide.
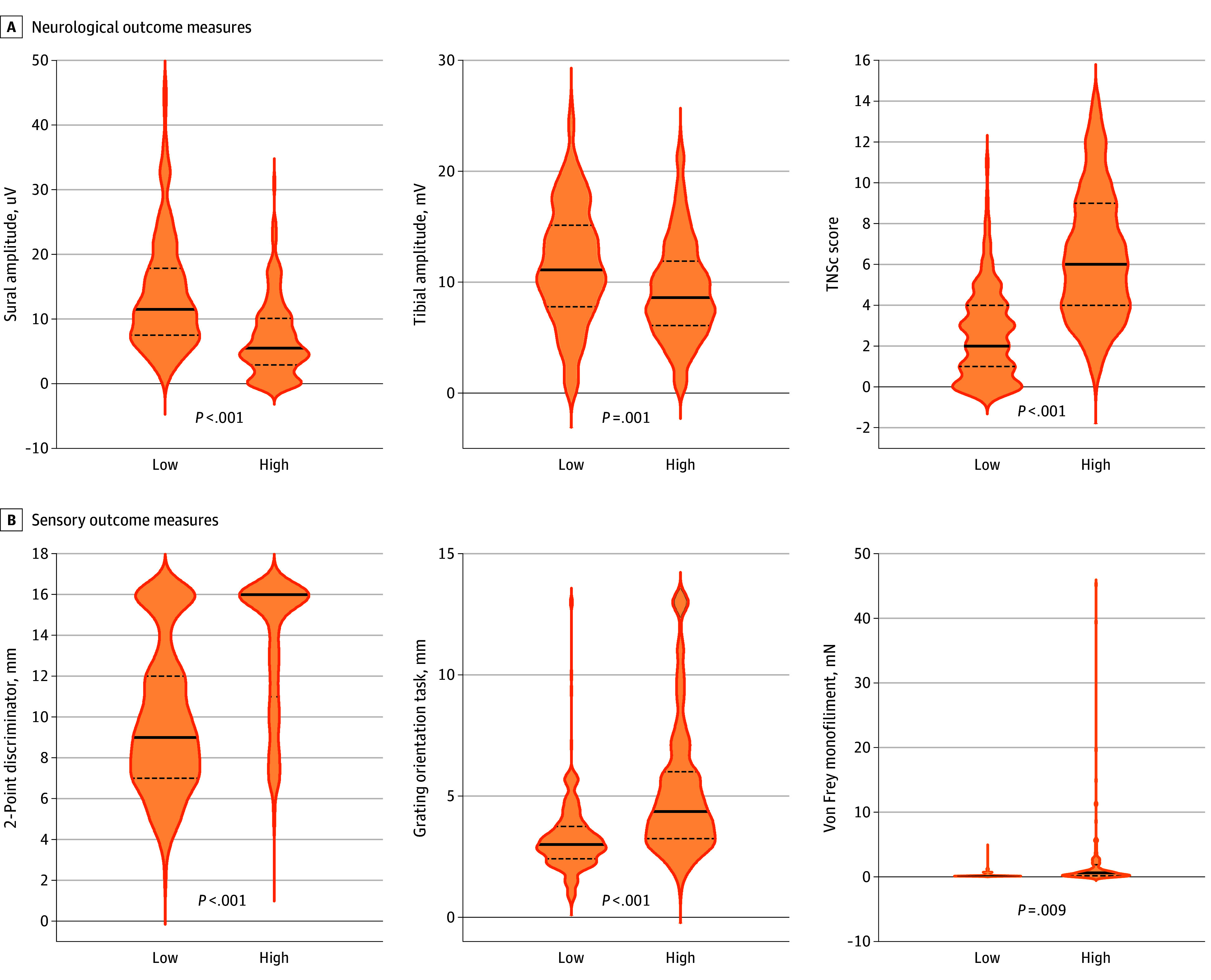
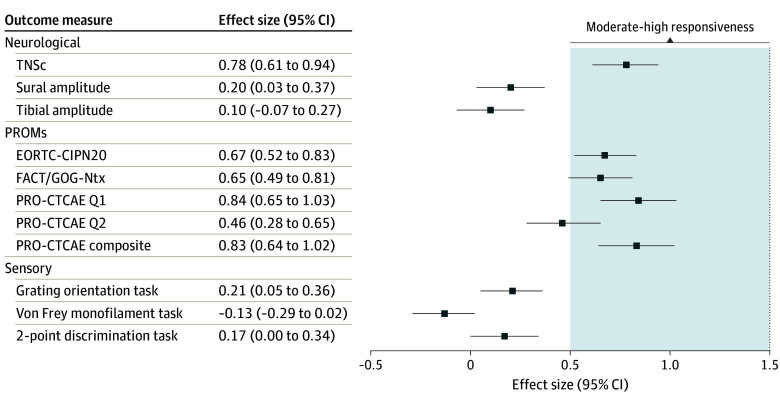
CIPN was assessed via PROMs (European Organization for Research and Treatment of Cancer Quality of Life Questionnaire [EORTC-CIPN20], Functional Assessment of Cancer Therapy/Gynecological Cancer Group Neurotoxicity Questionnaire (FACT/GOG-Ntx), and the patient-reported outcomes version of the Common Terminology Criteria for Adverse Events [PRO-CTCAE]), neurological and neurophysiological assessment (Total Neuropathy Score and sural and tibial compound nerve amplitudes), and sensory measures (Grating orientation, Von Frey monofilament, and 2-point discrimination tasks). Core measurement properties of CIPN outcome measures were evaluated. Convergent and known-groups validity was assessed cross-sectionally following treatment completion, and responsiveness was evaluated prospectively during treatment. Neurological, neurophysiological, and sensory outcome measure scores were compared between those who reported high and low levels of CIPN symptoms using linear regressions.
A total of 1033 participants (median [IQR] age, 61 [50-59] years; 676 female [65.4%]) were recruited to this study, incorporating 1623 assessments. PROMs demonstrated best ability to accurately assess CIPN (convergent validity), especially the PRO-CTCAE composite score (r = 0.85; P < .001) and EORTC-CIPN20 (r = 0.79; P < .001). PROMS also demonstrated the best ability to discriminate between CIPN severity (known-groups validity) and to detect changes at onset of CIPN development (responsiveness), especially for EORTC-CIPN20 (d = 0.67; 95% CI, 0.52-0.83), FACT/GOG-Ntx (d = 0.65; 95% CI, 0.49-0.81) and the PRO-CTCAE (d = 0.83; 95% CI, 0.64-1.02). Other measures did not achieve threshold for convergent validity (α < 0.7). Neurophysiological and sensory measures did not demonstrate acceptable responsiveness. In regression models, neurological, neurophysiological, and sensory outcome measures were significantly impaired in participants who reported high levels of CIPN symptoms compared with those who reported low levels of CIPN symptoms.
In this cohort study of 1033 cancer patients, PROMs were the only measures to satisfy all 3 core measurement property criteria (convergent validity, known-groups validity, and responsiveness). These findings suggest that adoption of PROMs in clinical practice can equip clinicians with valuable information in assessing CIPN morbidity.
化疗引起的周围神经病(CIPN)是癌症治疗的一种重要的不良反应。因此,CIPN 的评估在研究和临床环境中仍然至关重要。
比较各种患者报告的结局测量(PROM)与神经生理学和感觉功能测量作为 CIPN 评估的最佳方法。
设计、设置和参与者:这项队列研究使用双研究设计评估了接受神经毒性化疗的两组参与者。开始治疗的参与者在神经毒性治疗开始时、治疗中期和治疗结束时进行前瞻性评估。完成治疗长达 5 年的参与者进行横断面评估,并完成单一评估时间点。参与者从澳大利亚的肿瘤中心招募,招募时间为 2015 年 8 月至 2022 年 11 月。数据分析时间为 2023 年 2 月至 11 月。
包括紫杉烷类、铂类、长春碱类、蛋白酶体抑制剂和沙利度胺在内的神经毒性癌症治疗。
通过 PROM(欧洲癌症研究与治疗组织生活质量问卷 [EORTC-CIPN20]、癌症治疗功能评估/妇科癌症组神经毒性问卷 [FACT/GOG-Ntx] 和患者报告的不良事件通用术语标准 [PRO-CTCAE])、神经学和神经生理学评估(总神经评分和腓肠神经和胫骨复合神经幅度)以及感觉测量(光栅取向、冯弗雷单丝和两点区分任务)来评估 CIPN。评估了 CIPN 结局测量的核心测量特性。在完成治疗后进行横断面评估一致性和已知组有效性,在治疗期间进行前瞻性评估反应性。使用线性回归比较报告高和低 CIPN 症状水平的参与者之间的神经学、神经生理学和感觉测量结果评分。
这项研究共纳入了 1033 名参与者(中位数[IQR]年龄,61[50-59]岁;676 名女性[65.4%]),共进行了 1623 次评估。PROM 表现出准确评估 CIPN 的最佳能力(一致性),尤其是 PRO-CTCAE 综合评分(r=0.85;P<0.001)和 EORTC-CIPN20(r=0.79;P<0.001)。PROM 还表现出最佳的区分 CIPN 严重程度(已知组有效性)和检测 CIPN 发展起始时变化的能力(反应性),尤其是 EORTC-CIPN20(d=0.67;95%CI,0.52-0.83)、FACT/GOG-Ntx(d=0.65;95%CI,0.49-0.81)和 PRO-CTCAE(d=0.83;95%CI,0.64-1.02)。其他措施未达到一致性(α<0.7)的阈值。神经生理学和感觉测量未表现出可接受的反应性。在回归模型中,报告 CIPN 症状水平较高的参与者的神经学、神经生理学和感觉测量结果明显受损,而报告 CIPN 症状水平较低的参与者则没有。
在这项针对 1033 名癌症患者的队列研究中,PROM 是唯一满足所有 3 项核心测量特性标准(一致性、已知组有效性和反应性)的措施。这些发现表明,在临床实践中采用 PROM 可以为临床医生提供评估 CIPN 发病率的有价值的信息。