Division of Oncology, University of North Carolina, Chapel Hill, NC.
Alliance Statistics and Data Management Center, Mayo Clinic, Scottsdale, AZ.
J Clin Oncol. 2023 Jul 20;41(21):3724-3734. doi: 10.1200/JCO.23.00903. Epub 2023 Jun 4.
The standard of care for locally advanced rectal cancer in North America is neoadjuvant pelvic chemoradiation with fluorouracil (5FUCRT). Neoadjuvant chemotherapy with fluorouracil and oxaliplatin (FOLFOX) is an alternative that may spare patients the morbidity of radiation. Understanding the relative patient experiences with these options is necessary to inform treatment decisions.
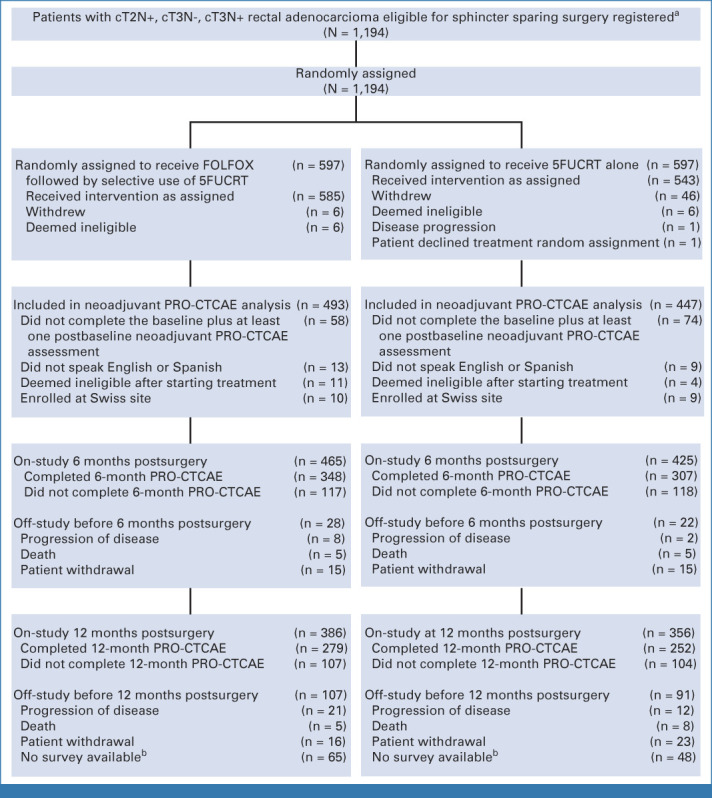
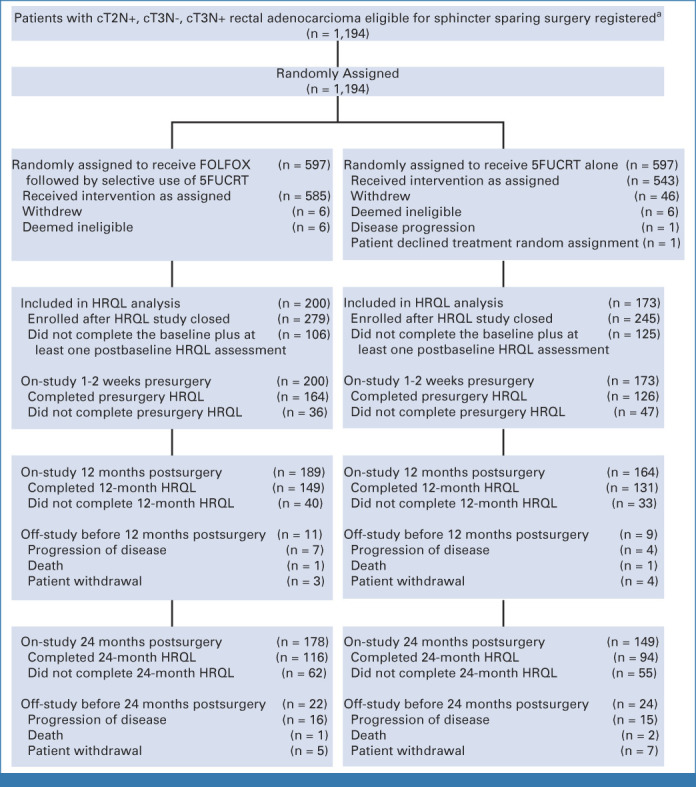
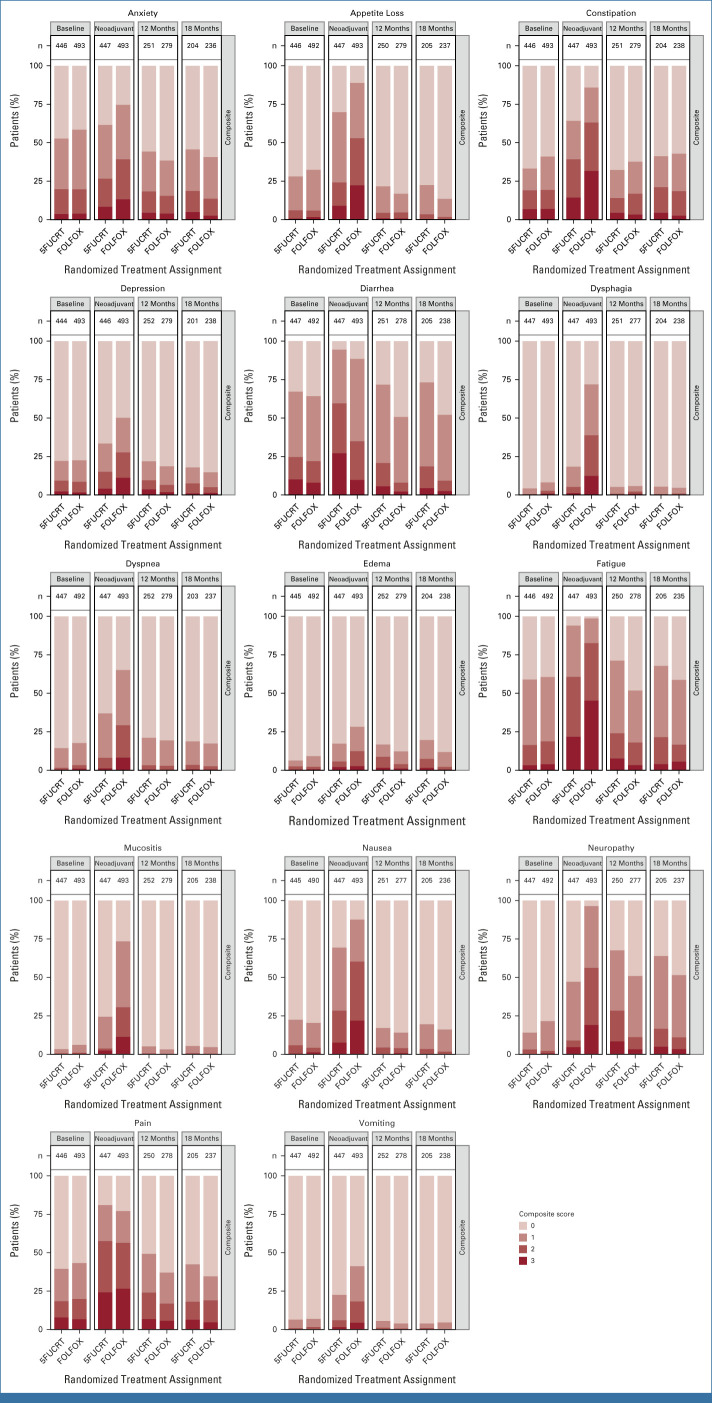
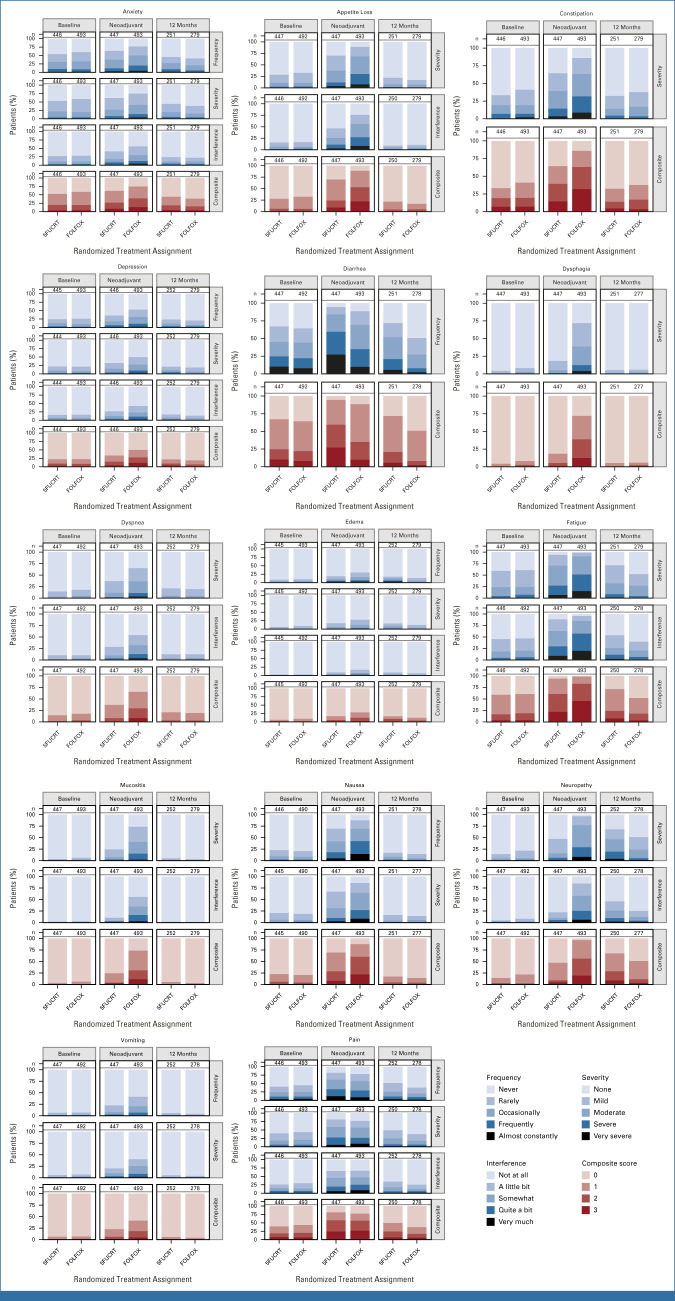
PROSPECT was a multicenter, unblinded, noninferiority, randomized trial of neoadjuvant FOLFOX versus 5FUCRT, which enrolled adults with rectal cancer clinically staged as T2N+, cT3N-, or cT3N+ who were candidates for sphincter-sparing surgery. Neoadjuvant FOLFOX was given in six cycles over 12 weeks, followed by surgery. Neoadjuvant 5FUCRT was delivered in 28 fractions over 5.5 weeks, followed by surgery. Adjuvant chemotherapy was suggested but not mandated in both groups. Enrolled patients were asked to provide patient-reported outcomes (PROs) at baseline, during neoadjuvant treatment, and at 12 months after surgery. PROs included 14 symptoms from the National Cancer Institute's Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). Additional PRO instruments measured bowel, bladder, sexual function, and health-related quality of life (HRQL).
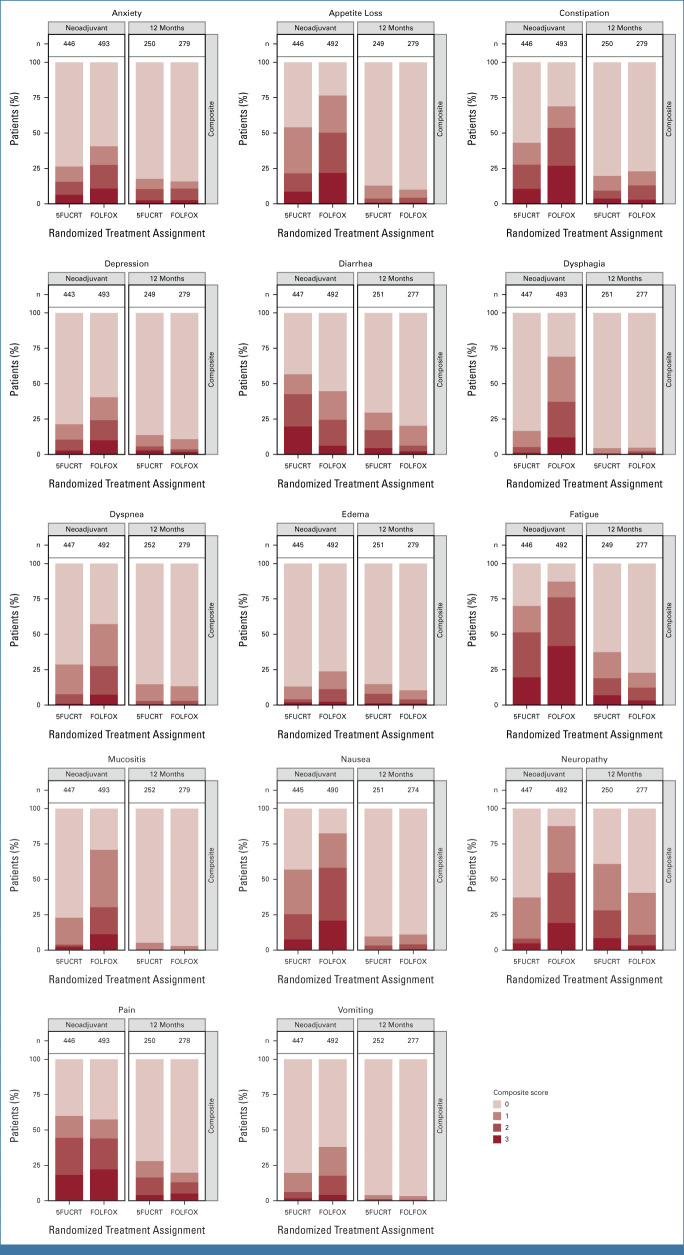
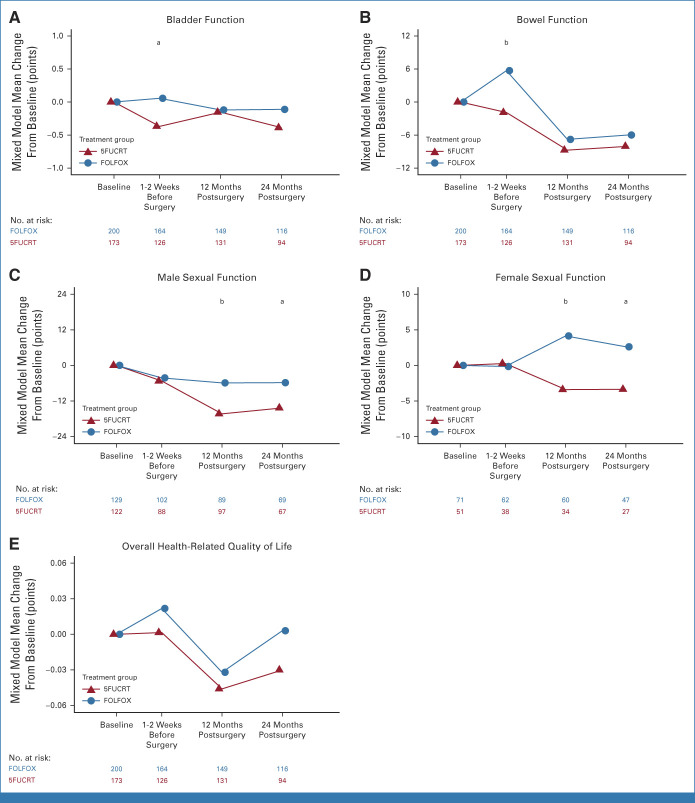
From June 2012 to December 2018, 1,194 patients were randomly assigned, 1,128 initiated treatment, and 940 contributed PRO-CTCAE data (493 FOLFOX; 447 5FUCRT). During neoadjuvant treatment, patients reported significantly lower rates of diarrhea and better overall bowel function with FOLFOX while anxiety, appetite loss, constipation, depression, dysphagia, dyspnea, edema, fatigue, mucositis, nausea, neuropathy, and vomiting were lower with 5FUCRT (all multiplicity adjusted < .05). At 12 months after surgery, patients randomly assigned to FOLFOX reported significantly lower rates of fatigue and neuropathy and better sexual function versus 5FUCRT (all multiplicity adjusted < .05). Neither bladder function nor HRQL differed between groups at any time point.
For patients with locally advanced rectal cancer choosing between neoadjuvant FOLFOX and 5FUCRT, the distinctive PRO profiles inform treatment selection and shared decision making.
北美局部晚期直肠癌的标准治疗方法是新辅助盆腔放化疗联合氟尿嘧啶(5FUCRT)。氟尿嘧啶和奥沙利铂联合新辅助化疗(FOLFOX)是一种替代方案,可避免患者遭受辐射的发病率。了解这些方案的相对患者体验对于制定治疗决策是必要的。
PROSPECT 是一项多中心、非盲、非劣效性、随机试验,比较新辅助 FOLFOX 与 5FUCRT,招募的患者为临床分期为 T2N+、cT3N-或 cT3N+的直肠癌成人,适合保留肛门手术。新辅助 FOLFOX 方案在 12 周内进行 6 个周期,随后进行手术。新辅助 5FUCRT 在 5.5 周内给予 28 个剂量,随后进行手术。两组均建议行辅助化疗,但不强制。入组患者在基线、新辅助治疗期间和手术后 12 个月被要求提供患者报告的结局(PROs)。PROs 包括来自国家癌症研究所患者报告结局版本的常见不良事件术语标准(PRO-CTCAE)的 14 个症状。其他 PRO 工具测量了肠道、膀胱、性功能和健康相关生活质量(HRQL)。
2012 年 6 月至 2018 年 12 月,共随机分配 1194 例患者,1128 例患者开始治疗,940 例患者提供 PRO-CTCAE 数据(493 例 FOLFOX;447 例 5FUCRT)。在新辅助治疗期间,FOLFOX 组患者报告腹泻发生率显著降低,整体肠道功能更好,而焦虑、食欲下降、便秘、抑郁、吞咽困难、呼吸困难、水肿、疲劳、黏膜炎、恶心、神经病变和呕吐发生率更低5FUCRT(所有多重调整均<0.05)。手术后 12 个月,随机分配至 FOLFOX 组的患者报告疲劳和神经病变发生率较低,性功能更好,与 5FUCRT 相比(所有多重调整均<0.05)。在任何时间点,膀胱功能或 HRQL 均无组间差异。
对于选择新辅助 FOLFOX 和 5FUCRT 的局部晚期直肠癌患者,独特的 PRO 特征可提供治疗选择和共同决策信息。