Santucci Domiziana, Ragone Raffaele, Vergantino Elva, Vaccarino Federica, Esperto Francesco, Prata Francesco, Scarpa Roberto Mario, Papalia Rocco, Beomonte Zobel Bruno, Grasso Francesco Rosario, Faiella Eliodoro
Department of Diagnostic Imaging, Campus Bio-Medico University of Rome, 00128 Rome, Italy.
Department of Urology, Campus Bio-Medico University of Rome, 00128 Rome, Italy.
Cancers (Basel). 2024 Jul 31;16(15):2731. doi: 10.3390/cancers16152731.
We aim to compare the performance of three different radiomics models (logistic regression (LR), random forest (RF), and support vector machine (SVM)) and clinical nomograms (Briganti, MSKCC, Yale, and Roach) for predicting lymph node involvement (LNI) in prostate cancer (PCa) patients.
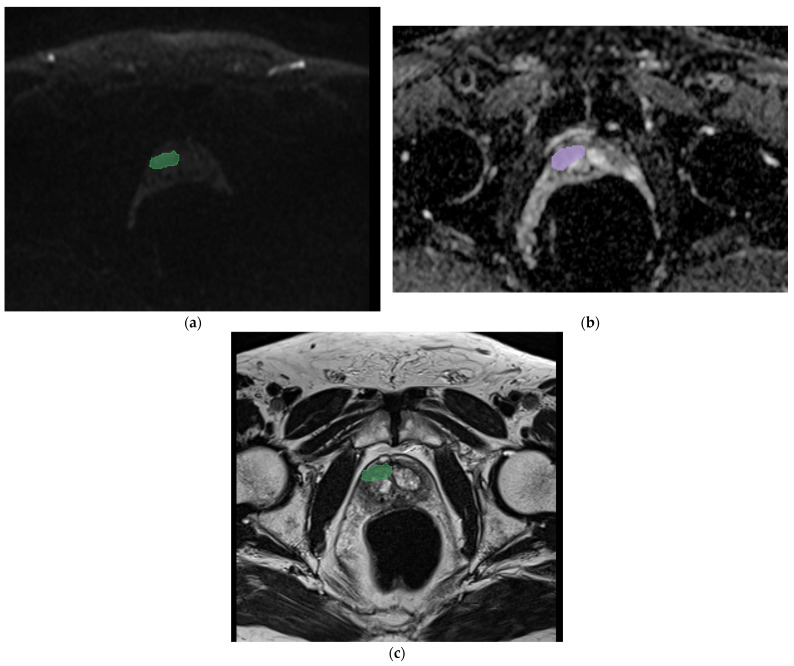
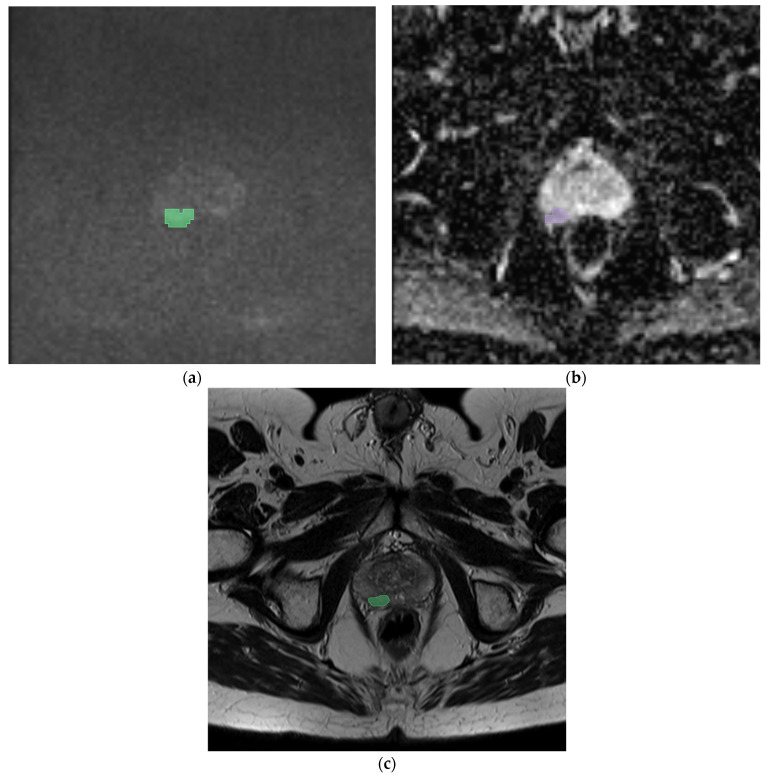
The retrospective study includes 95 patients who underwent mp-MRI and radical prostatectomy for PCa with pelvic lymphadenectomy. Imaging data (intensity in T2, DWI, ADC, and PIRADS), clinical data (age and pre-MRI PSA), histological data (Gleason score, TNM staging, histological type, capsule invasion, seminal vesicle invasion, and neurovascular bundle involvement), and clinical nomograms (Yale, Roach, MSKCC, and Briganti) were collected for each patient. Manual segmentation of the index lesions was performed for each patient using an open-source program (3D SLICER). Radiomic features were extracted for each segmentation using the Pyradiomics library for each sequence (T2, DWI, and ADC). The features were then selected and used to train and test three different radiomics models (LR, RF, and SVM) independently using ChatGPT software (v 4o). The coefficient value of each feature was calculated (significant value for coefficient ≥ ±0.5). The predictive performance of the radiomics models and clinical nomograms was assessed using accuracy and area under the curve (AUC) (significant value for ≤ 0.05). Thus, the diagnostic accuracy between the radiomics and clinical models were compared.
This study identified 343 features per patient (330 radiomics features and 13 clinical features). The most significant features were T2_nodulofirstordervariance and T2_nodulofirstorderkurtosis. The highest predictive performance was achieved by the RF model with DWI (accuracy 86%, AUC 0.89) and ADC (accuracy 89%, AUC 0.67). Clinical nomograms demonstrated satisfactory but lower predictive performance compared to the RF model in the DWI sequences.
Among the prediction models developed using integrated data (radiomics and semantics), RF shows slightly higher diagnostic accuracy in terms of AUC compared to clinical nomograms in PCa lymph node involvement prediction.
我们旨在比较三种不同的放射组学模型(逻辑回归(LR)、随机森林(RF)和支持向量机(SVM))以及临床列线图(布里甘蒂、纪念斯隆凯特琳癌症中心(MSKCC)、耶鲁和罗奇)在预测前列腺癌(PCa)患者淋巴结受累(LNI)方面的性能。
这项回顾性研究纳入了95例因PCa接受多参数磁共振成像(mp-MRI)和根治性前列腺切除术并伴有盆腔淋巴结清扫术的患者。收集了每位患者的影像数据(T2加权像、扩散加权成像(DWI)、表观扩散系数(ADC)和前列腺影像报告和数据系统(PIRADS)中的信号强度)、临床数据(年龄和MRI前前列腺特异性抗原(PSA))、组织学数据( Gleason评分、TNM分期、组织学类型、包膜侵犯、精囊侵犯和神经血管束受累情况)以及临床列线图(耶鲁、罗奇、MSKCC和布里甘蒂)。使用开源程序(3D Slicer)对每位患者的索引病变进行手动分割。使用Pyradiomics库针对每个序列(T2、DWI和ADC)为每个分割提取放射组学特征。然后使用ChatGPT软件(v 4o)对这些特征进行选择,并分别用于训练和测试三种不同的放射组学模型(LR、RF和SVM)。计算每个特征的系数值(系数的显著值≥±0.5)。使用准确率和曲线下面积(AUC)评估放射组学模型和临床列线图的预测性能(显著值为≤0.05)。因此,比较了放射组学模型和临床模型之间的诊断准确性。
本研究为每位患者识别出343个特征(330个放射组学特征和13个临床特征)。最显著的特征是T2_结节一阶方差和T2_结节一阶峰度。RF模型在DWI序列(准确率86%,AUC 0.89)和ADC序列(准确率89%,AUC 0.67)中实现了最高的预测性能。在DWI序列中,临床列线图显示出令人满意但低于RF模型的预测性能。
在使用综合数据(放射组学和语义学)开发的预测模型中,在PCa淋巴结受累预测方面,就AUC而言,RF显示出略高于临床列线图的诊断准确性。