Centre for Health Policy and Management, Trinity College Dublin, Dublin, Ireland.
LauraLynn Ireland's Children's Hospice and Children's Health Ireland at Tallaght, Dublin, Ireland.
BMC Palliat Care. 2024 Aug 22;23(1):212. doi: 10.1186/s12904-024-01539-8.
The number of children who require palliative care has been estimated to be as high as 21 million globally. Delivering effective children's palliative care (CPC) services requires accurate population-level information on current and future CPC need, but quantifying need is hampered by challenges in defining the population in need, and by limited available data. The objective of this paper is to summarise how population-level CPC need is defined, and quantified, in the literature.
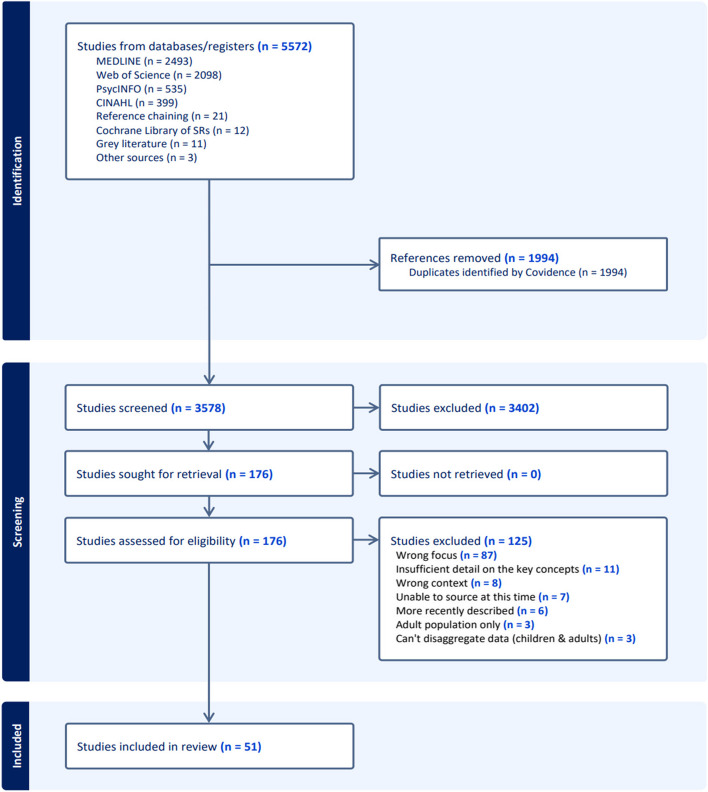
Scoping review performed in line with Joanna Briggs Institute methodology for scoping reviews and PRISMA-ScR guidelines. Six online databases (CINAHL, Cochrane Library, EMBASE, Medline, PsycINFO, and Web of Science), and grey literature, were searched.
literature published in English; 2008-2023 (Oct); including children aged 0-19 years; focused on defining and/or quantifying population-level need for palliative care.
Three thousand five hundred seventy-eight titles and abstracts initially reviewed, of which, 176 full-text studies were assessed for eligibility. Overall, 51 met the inclusion criteria for this scoping review. No universal agreement identified on how CPC need was defined in population-level policy and planning discussions. In practice, four key definitions of CPC need were found to be commonly applied in quantifying population-level need: (1) ACT/RCPCH (Association for Children with Life-Threatening or Terminal Conditions and their Families, and the Royal College of Paediatrics and Child Health) groups; (2) The 'Directory' of Life-Limiting Conditions; (3) 'List of Life-Limiting Conditions'; and (4) 'Complex Chronic Conditions'. In most cases, variations in data availability drove the methods used to quantify population-level CPC need and only a small proportion of articles incorporated measures of complexity of CPC need.
Overall, greater consistency in how CPC need is defined for policy and planning at a population-level is important, but with sufficient flexibility to allow for regional variations in epidemiology, demographics, and service availability. Improvements in routine data collection of a wide range of care complexity factors could facilitate estimation of population-level CPC need and ensure greater alignment with how need for CPC is defined at the individual-level in the clinical setting.
据估计,全球需要姑息治疗的儿童人数高达 2100 万。提供有效的儿童姑息治疗(CPC)服务需要准确了解当前和未来 CPC 需求的人口水平信息,但由于确定需求人群的挑战以及可用数据有限,因此量化需求受到阻碍。本文的目的是总结文献中如何定义和量化人口水平 CPC 需求。
根据 Joanna Briggs 研究所的范围综述方法和 PRISMA-ScR 指南进行范围综述。检索了六个在线数据库(CINAHL、Cochrane 图书馆、EMBASE、Medline、PsycINFO 和 Web of Science)和灰色文献。
发表于英文文献;2008-2023 年(10 月);包括 0-19 岁的儿童;重点关注姑息治疗的人口水平需求的定义和/或量化。
最初审查了 3578 个标题和摘要,其中 176 篇全文研究符合纳入标准。总体而言,有 51 项研究符合本范围综述的纳入标准。在人口水平的政策和规划讨论中,尚未就如何定义 CPC 需求达成普遍共识。实际上,在量化人口水平需求时,发现有四个常见的 CPC 需求的关键定义:(1)ACT/RCPCH(危及生命或终末期疾病儿童及其家庭协会和英国皇家儿科和儿童健康学院)组;(2)“目录”中的生命限制条件;(3)“生命限制条件清单”;(4)“复杂慢性疾病”。在大多数情况下,数据可用性的差异决定了用于量化人口水平 CPC 需求的方法,只有一小部分文章纳入了 CPC 需求复杂性的衡量标准。
总体而言,在人口层面为政策和规划定义 CPC 需求时,一致性更为重要,但需要具有足够的灵活性,以适应流行病学、人口统计学和服务可用性方面的区域差异。广泛收集各种护理复杂性因素的常规数据可以促进人口水平 CPC 需求的估算,并确保与临床环境中个人层面 CPC 需求的定义更加一致。