Rojas Juan C, Lyons Patrick G, Chhikara Kaveri, Chaudhari Vaishvik, Bhavani Sivasubramanium V, Nour Muna, Buell Kevin G, Smith Kevin D, Gao Catherine A, Amagai Saki, Mao Chengsheng, Luo Yuan, Barker Anna K, Nuppnau Mark, Beck Haley, Baccile Rachel, Hermsen Michael, Liao Zewei, Park-Egan Brenna, Carey Kyle A, Hochberg Chad H, Ingraham Nicholas E, Parker William F
Division of Pulmonology, Critical Care, and Sleep Medicine, Rush University, Chicago, IL.
Department of Medicine, Oregon Health & Science University, Portland, OR.
medRxiv. 2024 Sep 4:2024.09.04.24313058. doi: 10.1101/2024.09.04.24313058.
Critical illness, or acute organ failure requiring life support, threatens over five million American lives annually. Electronic health record (EHR) data are a source of granular information that could generate crucial insights into the nature and optimal treatment of critical illness. However, data management, security, and standardization are barriers to large-scale critical illness EHR studies.
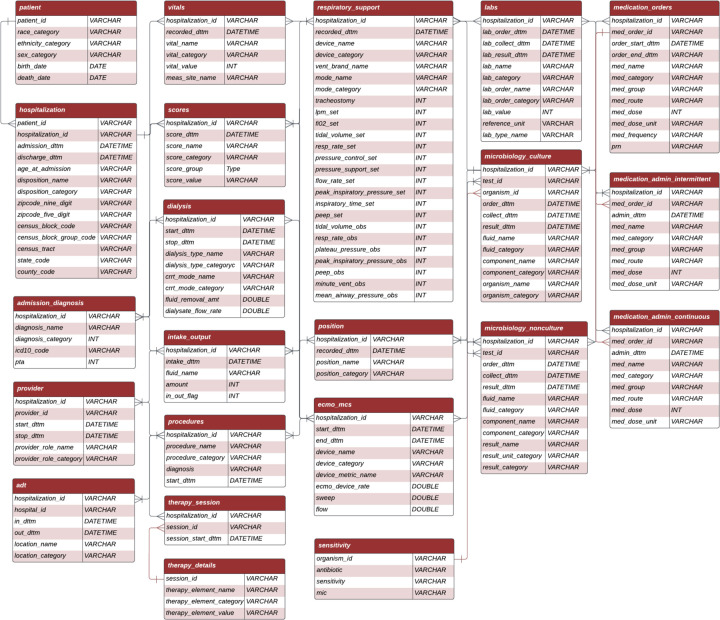
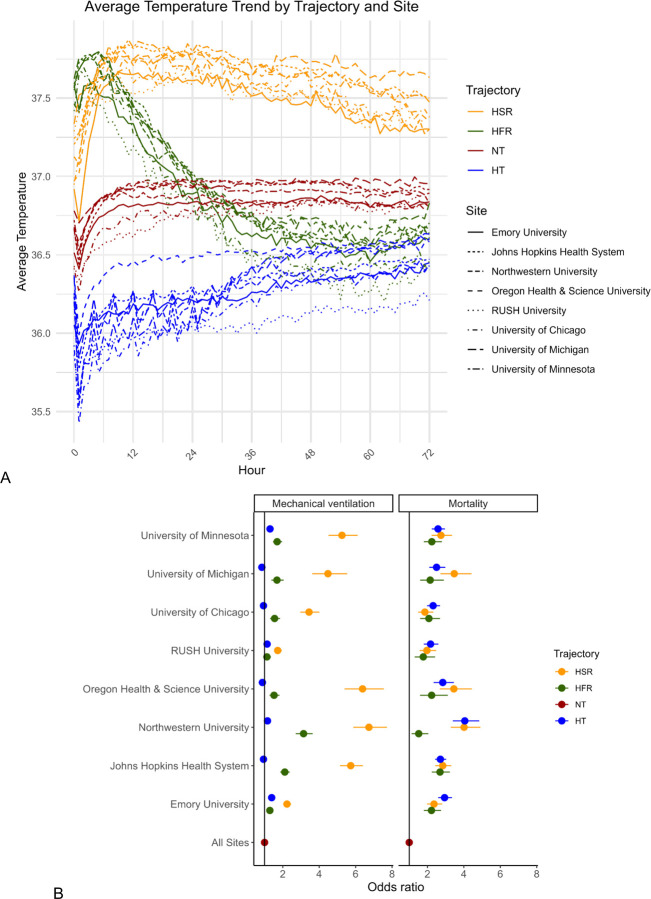
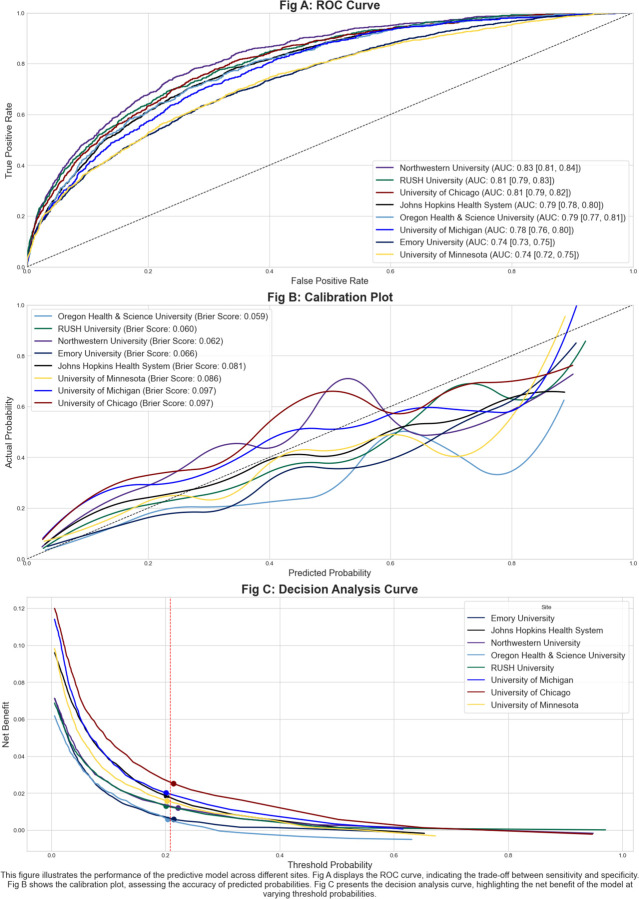
A consortium of critical care physicians and data scientists from eight US healthcare systems developed the Common Longitudinal Intensive Care Unit (ICU) data Format (CLIF), an open-source database format that harmonizes a minimum set of ICU Data Elements for use in critical illness research. We created a pipeline to process adult ICU EHR data at each site. After development and iteration, we conducted two proof-of-concept studies with a federated research architecture: 1) an external validation of an in-hospital mortality prediction model for critically ill patients and 2) an assessment of 72-hour temperature trajectories and their association with mechanical ventilation and in-hospital mortality using group-based trajectory models.
We converted longitudinal data from 94,356 critically ill patients treated in 2020-2021 (mean age 60.6 years [standard deviation 17.2], 30% Black, 7% Hispanic, 45% female) across 8 health systems and 33 hospitals into the CLIF format, The in-hospital mortality prediction model performed well in the health system where it was derived (0.81 AUC, 0.06 Brier score). Performance across CLIF consortium sites varied (AUCs: 0.74-0.83, Brier scores: 0.06-0.01), and demonstrated some degradation in predictive capability. Temperature trajectories were similar across health systems. Hypothermic and hyperthermic-slow-resolver patients consistently had the highest mortality.
CLIF facilitates efficient, rigorous, and reproducible critical care research. Our federated case studies showcase CLIF's potential for disease sub-phenotyping and clinical decision-support evaluation. Future applications include pragmatic EHR-based trials, target trial emulations, foundational multi-modal AI models of critical illness, and real-time critical care quality dashboards.
危重病,即需要生命支持的急性器官衰竭,每年威胁着超过500万美国人的生命。电子健康记录(EHR)数据是细粒度信息的来源,可为危重病的本质和最佳治疗提供关键见解。然而,数据管理、安全性和标准化是大规模危重病EHR研究的障碍。
来自美国八个医疗系统的重症监护医师和数据科学家组成的联盟开发了通用纵向重症监护病房(ICU)数据格式(CLIF),这是一种开源数据库格式,用于协调一组最低限度的ICU数据元素,以用于危重病研究。我们创建了一个管道来处理每个站点的成人ICU EHR数据。经过开发和迭代,我们使用联合研究架构进行了两项概念验证研究:1)对危重病患者院内死亡率预测模型的外部验证,以及2)使用基于组的轨迹模型评估72小时体温轨迹及其与机械通气和院内死亡率的关联。
我们将2020年至2021年在8个医疗系统和33家医院接受治疗的94356名危重病患者(平均年龄60.6岁[标准差17.2],30%为黑人,7%为西班牙裔,45%为女性)的纵向数据转换为CLIF格式。院内死亡率预测模型在其推导的医疗系统中表现良好(曲线下面积[AUC]为0.81,Brier评分0.06)。CLIF联盟各站点的表现各不相同(AUC:0.74 - 0.83,Brier评分:0.06 - 0.01),并且预测能力有所下降。各医疗系统的体温轨迹相似。体温过低和体温过高且恢复缓慢的患者死亡率始终最高。
CLIF有助于高效、严谨且可重复的重症监护研究。我们的联合案例研究展示了CLIF在疾病亚表型分析和临床决策支持评估方面的潜力。未来的应用包括基于EHR的务实试验、目标试验模拟、危重病的基础多模态人工智能模型以及实时重症监护质量仪表板。