Department of Neurosurgery, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People's Republic of China.
Department of Operation Anaesthesia, University-Town Hospital of Chongqing Medical University, Chongqing, People's Republic of China.
Sci Rep. 2024 Sep 18;14(1):21802. doi: 10.1038/s41598-024-72142-3.
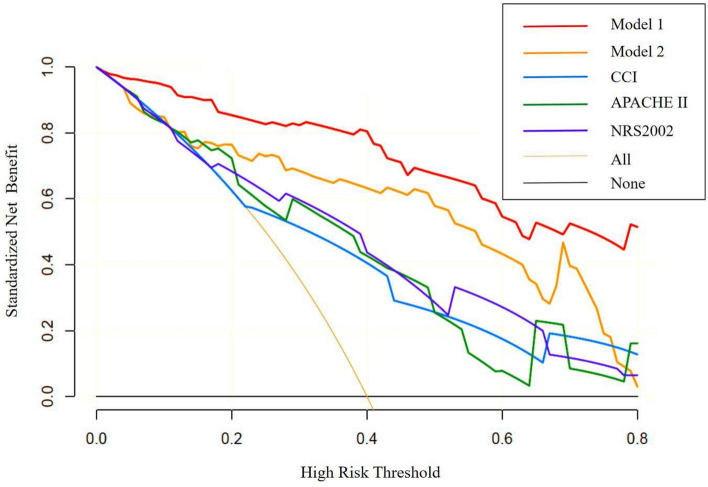
The purpose of this study was to investigate early stage dynamic changes in relevant indicators in neurocritical patients to identify biomarkers that can predict a poor prognosis at an early stage (1-4 days after admission). This study retrospectively collected clinical data, inflammatory indicators, and nutritional indicators from 77 patients at the neurology intensive care unit. The 3-month modified Rankin scale score was used as the outcome indicator. A linear mixed model was used to analyze changes in inflammatory indicators and nutritional indicators in neurocritical patients over time from 1-4 days after admission. Logistic regression was used to determine the independent risk factors for a poor prognosis in neurocritical patients and to construct a predictive model. The predictive efficacy of the model was verified using leave-one-out cross-validation and decision curve analysis methods. The analysis results showed that 1-4 days after admission, the inflammatory indicators of white blood cell and absolute monocyte counts and the nutritional indicators of body cell mass(BCM), fat-free mass, body cell mass/phase angle (BCM/PA), intracellular water, extracellular water, and skeletal muscle index increased overall, while the nutritional indicators of albumin and visceral fat area decreased overall. The logistic multivariate regression model showed that the Charlson comorbidity index (CCI) (odds ratio (OR) = 2.526, 95% CI [1.202, 5.308]), hemoglobin (Hb)(on admission)-Hb(min) (OR = 1.049, 95% CI [1.015, 1.083), BCM(on admission) (OR = 0.794, 95% CI [0.662, 0.952]), and the change in BCM/PA 1-4 days after admission (OR = 1.157, 95% CI [1.070, 1.252]) were independent risk factors for a poor prognosis in neurocritical patients. The predictive analysis showed that the predictive power of Model 1 with BCM/PA (area under the curve (AUC) = 0.95, 95% CI (0.90, 0.99)) was 93%, 65%, 141%, and 133% higher than that of Model 2 without BCM/PA, the CCI, the APACHE II score, and the NRS2002 score (all P < 0.05), respectively. The CCI, Hb(on admission)-Hb(min), BCM(on admission), and an increase in BCM/PA 1-4 days after admission were independently associated with a poor prognosis in neurocritical patients. Of these variables, BCM/PA may be a valid indicator for early stage prediction of a poor prognosis in neurocritical patients.
本研究旨在探讨神经危重症患者早期相关指标的动态变化,寻找能够早期(入院后 1-4 天)预测不良预后的生物标志物。本研究回顾性收集了神经内科重症监护病房 77 例患者的临床资料、炎症指标和营养指标。采用改良的 3 个月 Rankin 量表评分作为结局指标。采用线性混合模型分析神经危重症患者入院后 1-4 天炎症指标和营养指标的时间变化。采用 logistic 回归分析确定神经危重症患者不良预后的独立危险因素,并构建预测模型。采用留一法交叉验证和决策曲线分析方法验证模型的预测效能。分析结果显示,入院后 1-4 天,白细胞和绝对单核细胞计数等炎症指标以及体细胞质量(BCM)、去脂体重、BCM/相位角(BCM/PA)、细胞内水、细胞外水和骨骼肌指数等营养指标总体呈上升趋势,而白蛋白和内脏脂肪面积等营养指标总体呈下降趋势。logistic 多因素回归模型显示,Charlson 合并症指数(CCI)(比值比(OR)=2.526,95%置信区间(CI)[1.202,5.308])、入院时血红蛋白(Hb)-最低 Hb 值(OR=1.049,95%CI[1.015,1.083])、入院时 BCM(OR=0.794,95%CI[0.662,0.952])和入院后 1-4 天 BCM/PA 变化(OR=1.157,95%CI[1.070,1.252])是神经危重症患者不良预后的独立危险因素。预测分析显示,加入 BCM/PA 的模型 1(曲线下面积(AUC)=0.95,95%CI[0.90,0.99])的预测效能分别比模型 2(不包含 BCM/PA、CCI、APACHE II 评分和 NRS2002 评分)、CCI、APACHE II 评分和 NRS2002 评分高 93%、65%、141%和 133%(均 P<0.05)。CCI、入院时 Hb-Hb 最低值、入院时 BCM 和入院后 1-4 天 BCM/PA 增加与神经危重症患者不良预后独立相关。其中,BCM/PA 可能是神经危重症患者不良预后早期预测的有效指标。