Choudhary Tilendra, Upadhyaya Pulakesh, Davis Carolyn M, Yang Philip, Tallowin Simon, Lisboa Felipe A, Schobel Seth A, Coopersmith Craig M, Elster Eric A, Buchman Timothy G, Dente Christopher J, Kamaleswaran Rishikesan
Department of Surgery, Duke University School of Medicine, Durham, NC, 27707, USA.
Department of Surgery, Emory University School of Medicine, Atlanta, GA, 30332, USA.
Crit Care. 2024 Oct 1;28(1):321. doi: 10.1186/s13054-024-05061-4.
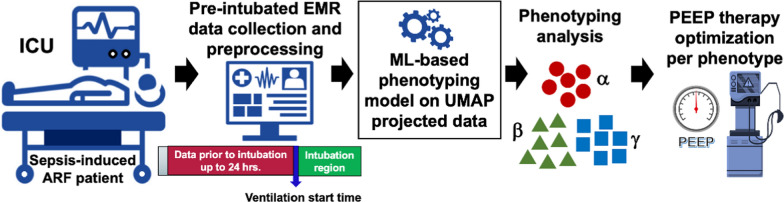
Septic patients who develop acute respiratory failure (ARF) requiring mechanical ventilation represent a heterogenous subgroup of critically ill patients with widely variable clinical characteristics. Identifying distinct phenotypes of these patients may reveal insights about the broader heterogeneity in the clinical course of sepsis, considering multi-organ dynamics. We aimed to derive novel phenotypes of sepsis-induced ARF using observational clinical data and investigate the generalizability of the derived phenotypes.
We performed a multi-center retrospective study of ICU patients with sepsis who required mechanical ventilation for ≥ 24 h. Data from two different high-volume academic hospital centers were used, where all phenotypes were derived in MICU of Hospital-I (N = 3225). The derived phenotypes were validated in MICU of Hospital-II (N = 848), SICU of Hospital-I (N = 1112), and SICU of Hospital-II (N = 465). Clinical data from 24 h preceding intubation was used to derive distinct phenotypes using an explainable machine learning-based clustering model interpreted by clinical experts.
Four distinct ARF phenotypes were identified: A (severe multi-organ dysfunction (MOD) with a high likelihood of kidney injury and heart failure), B (severe hypoxemic respiratory failure [median P/F = 123]), C (mild hypoxia [median P/F = 240]), and D (severe MOD with a high likelihood of hepatic injury, coagulopathy, and lactic acidosis). Patients in each phenotype showed differences in clinical course and mortality rates despite similarities in demographics and admission co-morbidities. The phenotypes were reproduced in external validation utilizing the MICU of Hospital-II and SICUs from Hospital-I and -II. Kaplan-Meier analysis showed significant difference in 28-day mortality across the phenotypes (p < 0.01) and consistent across MICU and SICU of both Hospital-I and -II. The phenotypes demonstrated differences in treatment effects associated with high positive end-expiratory pressure (PEEP) strategy.
The phenotypes demonstrated unique patterns of organ injury and differences in clinical outcomes, which may help inform future research and clinical trial design for tailored management strategies.
发生急性呼吸衰竭(ARF)且需要机械通气的脓毒症患者是危重症患者中的一个异质性亚组,其临床特征差异很大。考虑到多器官动态变化,识别这些患者的不同表型可能会揭示脓毒症临床病程中更广泛的异质性。我们旨在利用观察性临床数据推导脓毒症诱导的ARF的新表型,并研究推导表型的普遍性。
我们对需要机械通气≥24小时的脓毒症ICU患者进行了一项多中心回顾性研究。使用了来自两个不同的高容量学术医院中心的数据,所有表型均在医院I的MICU中推导得出(N = 3225)。推导的表型在医院II的MICU(N = 848)、医院I的SICU(N = 1112)和医院II的SICU(N = 465)中进行了验证。使用插管前24小时的临床数据,通过临床专家解释的基于可解释机器学习的聚类模型推导不同的表型。
识别出四种不同的ARF表型:A(严重多器官功能障碍(MOD),伴有肾损伤和心力衰竭的高可能性)、B(严重低氧性呼吸衰竭[中位数P/F = 123])、C(轻度缺氧[中位数P/F = 240])和D(严重MOD,伴有肝损伤、凝血病和乳酸性酸中毒的高可能性)。尽管各表型患者在人口统计学和入院合并症方面相似,但临床病程和死亡率存在差异。这些表型在利用医院II的MICU以及医院I和II的SICU进行的外部验证中得到了重现。Kaplan-Meier分析显示各表型在28天死亡率上存在显著差异(p < 0.01),并且在医院I和II的MICU和SICU中一致。这些表型在与高呼气末正压(PEEP)策略相关的治疗效果上表现出差异。
这些表型展示了独特的器官损伤模式和临床结局差异,这可能有助于为未来针对个体化管理策略的研究和临床试验设计提供信息。