Bai Huihui, Niu Dan, Li Boling, Zong Yuan, Wang Yan
Department of Intensive Care Unit, Shaanxi Province People's Hospital, Xi An, China.
Sci Rep. 2025 Jul 31;15(1):27972. doi: 10.1038/s41598-025-12853-3.
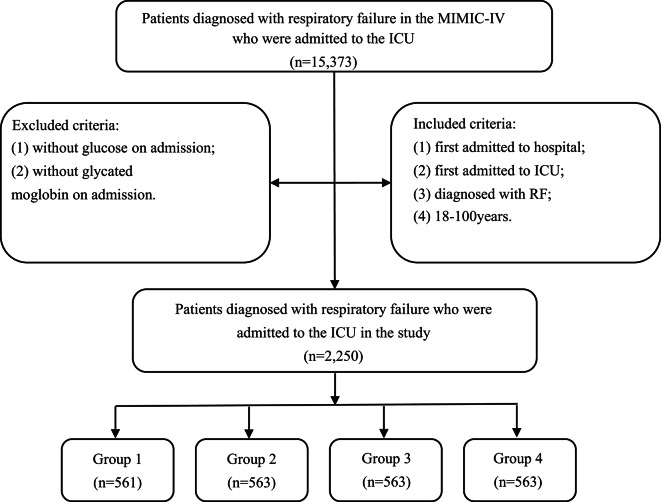
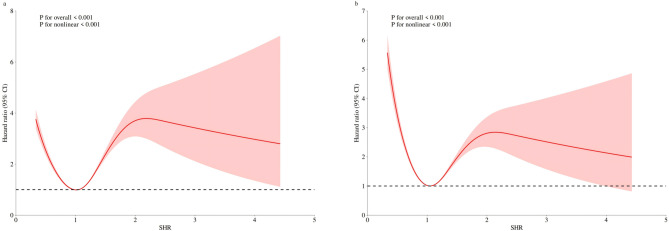
The stress hyperglycemia ratio (SHR) represents an emerging biomarker linked to poor clinical outcomes. However, its association with fatal outcomes in patients experiencing respiratory failure (RF) remains poorly understood. This research was designed to evaluate the utility of SHR in predicting both in-hospital mortality and intensive care unit (ICU) mortality among RF patients. This retrospective cohort analysis utilized data from the MIMIC-IV version 3.0 database. Patients diagnosed with RF in the ICU were divided into four groups according to the SHR index quartiles (group1, group2, group3, and group4), and the outcomes were in-hospital and ICU mortality. Survival outcomes among different groups were analyzed through Kaplan-Meier curves. Based on the results of the schoenfeld residual test, choose the Cox model or the model with the time interaction term to report the association between SHR and the outcome. Furthermore, restricted cubic splines analyses were conducted to explore potential non-linear relationships of SHR with both in-hospital and ICU mortality. This study enrolled 2,250 participants, demonstrating in-hospital mortality and ICU mortality rates of 23.91% and 14.31%, respectively. Kaplan-Meier analysis revealed that the group4 exhibited the lowest survival rates (P < 0.001). Through multivariate Cox regression, when comparing the group1 to the group4, three analytical models consistently showed increased in-hospital and ICU mortality in group4. The time interaction model revealed significant increases in hospital mortality risk across SHR quartiles compared to group1. Specifically, in model1, group2 showed a 62%-69% higher risk (HR = 1.69, 95% CI: 1.17-2.44), group3 exhibited a 358%-370% higher risk (HR = 4.58, 95% CI: 1.83-11.5) ,while group4 demonstrated exponential risk escalation. All quartile groups exhibited a daily risk attenuation of approximately 57% (time interaction term HR = 0.43, all p < 0.001). The associations remained consistent after adjusting the variables in models 2 and 3. In contrast, no significant risk association was observed between SHR and ICU mortality in the time interaction model. Besides, a U-shaped relationship was observed between SHR and both in-hospital mortality and ICU mortality. The study revealed that elevated SHR levels in ICU-admitted RF patients were significantly associated with increased risks of in-hospital mortality. Clinicians should closely monitor patients with high admission SHR values, especially patients in the highest SHR quantile (Q4 group) during the early admission period, underscoring the need for prioritized clinical intervention in this high-risk population.
应激性高血糖比值(SHR)是一种与不良临床结局相关的新兴生物标志物。然而,其与呼吸衰竭(RF)患者死亡结局的关联仍知之甚少。本研究旨在评估SHR在预测RF患者院内死亡率和重症监护病房(ICU)死亡率方面的效用。这项回顾性队列分析使用了MIMIC-IV版本3.0数据库中的数据。在ICU中被诊断为RF的患者根据SHR指数四分位数分为四组(第1组、第2组、第3组和第4组),结局指标为院内死亡率和ICU死亡率。通过Kaplan-Meier曲线分析不同组之间的生存结局。基于Schoenfeld残差检验结果,选择Cox模型或带有时间交互项的模型来报告SHR与结局之间的关联。此外,进行了受限立方样条分析以探索SHR与院内死亡率和ICU死亡率之间潜在的非线性关系。本研究纳入了2250名参与者,院内死亡率和ICU死亡率分别为23.91%和14.31%。Kaplan-Meier分析显示,第4组的生存率最低(P<0.001)。通过多变量Cox回归分析,将第1组与第4组进行比较时,三个分析模型均一致显示第4组的院内死亡率和ICU死亡率增加。时间交互模型显示,与第1组相比,SHR四分位数分组的医院死亡风险显著增加。具体而言,在模型1中,第2组的风险高62%-69%(HR=1.69,95%CI:1.17-2.44),第3组的风险高358%-370%(HR=4.58,95%CI:1.83-11.5),而第4组的风险呈指数级上升。所有四分位数分组的每日风险衰减约为57%(时间交互项HR=0.43,所有p<0.001)。在模型2和3中调整变量后,这些关联仍然一致。相比之下,时间交互模型中未观察到SHR与ICU死亡率之间存在显著的风险关联。此外,观察到SHR与院内死亡率和ICU死亡率之间呈U形关系。该研究表明,入住ICU的RF患者SHR水平升高与院内死亡风险增加显著相关。临床医生应密切监测入院时SHR值高的患者,尤其是入院早期处于SHR最高四分位数(Q4组)的患者,这突出了对这一高危人群进行优先临床干预的必要性。