Young Bethany C, Ehntholt Mikel S, Kumar Monisha A
From the Department of Nursing (B.C.Y.), Hospital of the University of Pennsylvania, Philadelphia; Department of Critical Care Medicine (M.S.E.), Virtua Health, Camden, NJ; and Department of Neurology (M.S.E., M.A.K.), University of Pennsylvania, Philadelphia.
Neurol Educ. 2024 Apr 12;3(2):e200128. doi: 10.1212/NE9.0000000000200128. eCollection 2024 Jun.
Neurocritical care (NCC) is a niche clinical subspecialty dependent on interdisciplinary cohesion to operate in critical situations. Team cohesion in an intensive care unit (ICU) depends not only on technical skills or medical knowledge but also on nontechnical skills such as teamwork, communication, and leadership. Developing and practicing these skills as an interdisciplinary team is not standard in most professional training programs.
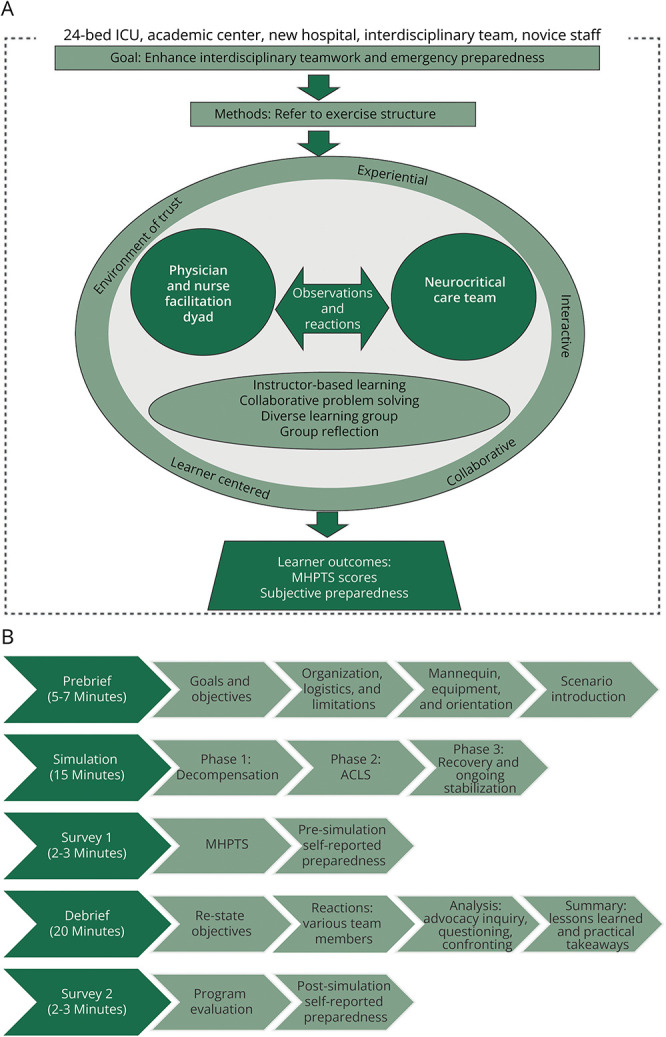
This project aimed to (1) design and implement a NCC in situ simulation program aimed at practicing teamwork, (2) demonstrate feasibility and acceptability of recurring in situ simulations, and (3) assess baseline teamwork scores and clinician preparedness to respond to a clinical emergency.
The NLN Jeffries Simulation Theory was used to guide the simulation program design. A 1-year pilot project consisted of monthly NCC in situ simulations. Debriefing with Good Judgment was used to guide postsimulation reflection. Feasibility was evaluated by participation metrics and simulation schedule adherence. Acceptability was assessed through postsimulation evaluations. Teamwork and preparedness were measured using the Mayo High Performance Teamwork Scale (MHPTS) and 10-point Likert scale, respectively. Statistical comparison of MHPTS scores between disciplines and preparedness before vs after simulation was conducted.
In 1 year, we conducted 12 in situ simulations, with 167 simulation learner encounters, representing 95 unique learners and 72% of our core NCC team (i.e., nurses, advanced practice providers [APPs], fellows, faculty). Analysis of program evaluations (84% survey completion rate) showed that 91% of all learners strongly agreed that the simulation provided an experiential, collaborative, trusting, and learner-centered environment. Overall, MHPTS scores were similar between disciplines, although in pairwise comparison, pharmacists rated teamwork significantly lower than both nurses ( = 0.01) and APPs ( = 0.004). Learners rated their preparedness to respond to a clinical emergency significantly higher after the simulation ( < 0.001).
In situ simulation training is a feasible and acceptable method to introduce teamwork training into ICU culture. Team-based simulation improves self-reported preparation to respond to clinical emergencies. Simulation training that takes place in the clinical setting provides a powerful tool for enhancing teaching and addressing patient care gaps.
神经重症监护(NCC)是一个细分的临床亚专业,在危急情况下的运作依赖于跨学科的紧密协作。重症监护病房(ICU)中的团队凝聚力不仅取决于技术技能或医学知识,还取决于团队合作、沟通和领导力等非技术技能。作为一个跨学科团队培养和实践这些技能在大多数专业培训项目中并非标准做法。
本项目旨在(1)设计并实施一个旨在实践团队合作的NCC现场模拟项目,(2)证明反复进行现场模拟的可行性和可接受性,(3)评估团队合作的基线得分以及临床医生应对临床紧急情况的准备情况。
使用NLN杰弗里斯模拟理论指导模拟项目设计。一个为期1年的试点项目包括每月一次的NCC现场模拟。采用“良好判断”进行复盘以指导模拟后的反思。通过参与指标和模拟计划遵守情况评估可行性。通过模拟后评估来评估可接受性。分别使用梅奥高效团队合作量表(MHPTS)和10点李克特量表测量团队合作和准备情况。对不同学科之间的MHPTS得分以及模拟前后的准备情况进行统计比较。
在1年时间里,我们进行了12次现场模拟,有167次模拟学习者参与,涉及95名不同的学习者以及我们核心NCC团队的72%(即护士、高级实践提供者[APPs]、研究员、教员)。对项目评估的分析(调查完成率为84%)表明,91%的学习者强烈同意模拟提供了一个体验式、协作式、信任式且以学习者为中心的环境。总体而言,不同学科之间的MHPTS得分相似,不过在两两比较中,药剂师对团队合作的评分显著低于护士( = 0.01)和APPs( = 0.004)。模拟后学习者对其应对临床紧急情况的准备情况评分显著更高( < 0.001)。
现场模拟培训是将团队合作培训引入ICU文化的一种可行且可接受的方法。基于团队的模拟提高了自我报告的应对临床紧急情况的准备程度。在临床环境中进行的模拟培训为加强教学和弥补患者护理差距提供了一个有力工具。