Department of Cardiology and Geriatrics, Kochi Medical School, Kochi University, Oko-Cho, Nankoku-Shi, Kochi, 783-8505, Japan.
Department of Clinical Laboratory, Kochi Medical School Hospital, Kochi, Japan.
Cardiovasc Ultrasound. 2024 Oct 7;22(1):12. doi: 10.1186/s12947-024-00331-1.
Echocardiography remains the reference-standard imaging technique for assessing valvular heart disease (VHD), but artifacts like the 'color Doppler stripe' can complicate diagnosis. This artifact is not widely recognized and can mimic severe VHD, leading to potential misdiagnoses. We present two cases where color Doppler stripes mimicked severe VHD, highlighting the need for awareness and accurate interpretation in echocardiographic assessments.
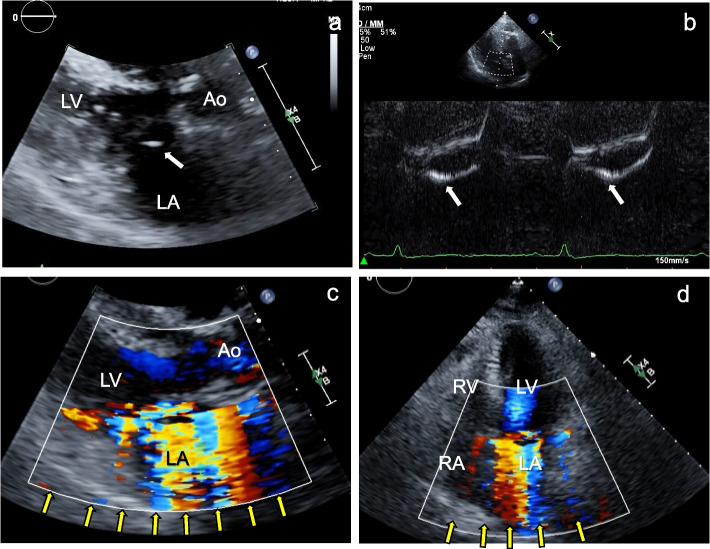
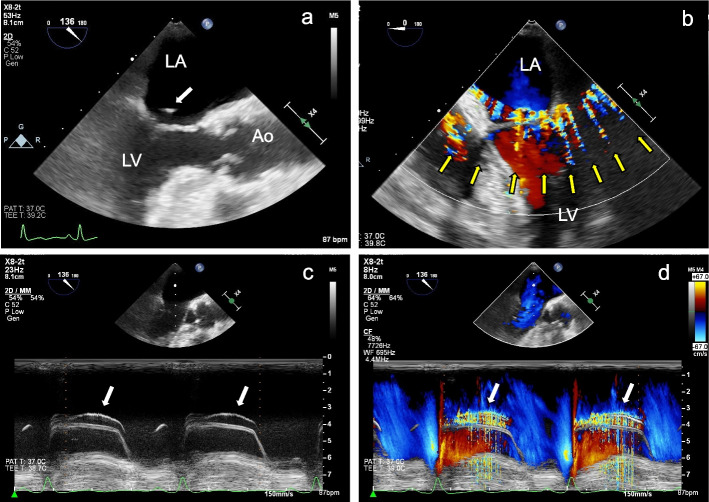
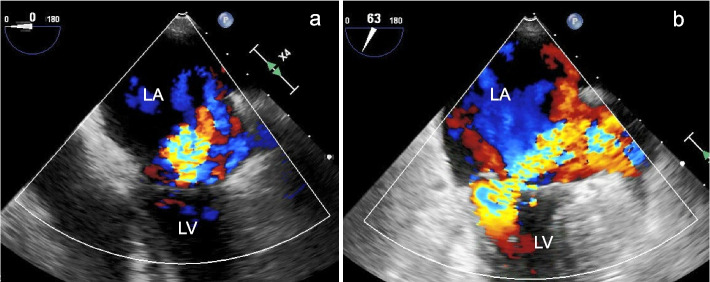
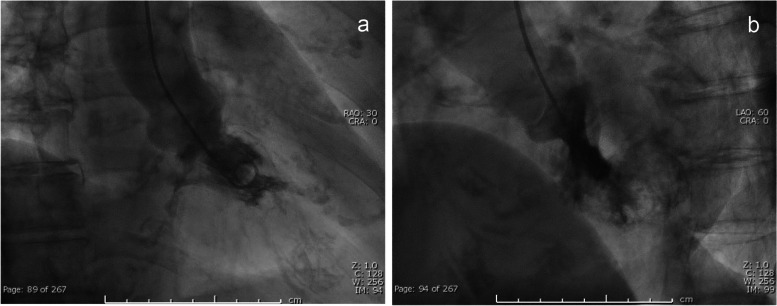
Case 1: An 85-year-old patient was referred for mitral valve surgery due to suspected severe mitral regurgitation (MR). Upon evaluation, transthoracic echocardiography (TTE) showed mitral valve prolapse (P3) and a high-echoic, vibrating structure attached to the mitral valve, indicative of chordal rupture. Color Doppler echocardiography revealed strong systolic signals in the left atrium, mimicking severe MR. Transesophageal echocardiography (TEE) also detected the vibrating structure and color Doppler stripes in the left atrium, left ventricle, and outside the cardiac chambers. The PISA method on TEE indicated moderate MR and left ventriculography showed Sellers grade II MR. The artifact was identified as color Doppler stripes caused by the vibrating high-echoic structure from the ruptured chorda. Case 2: A 64-year-old patient with severe aortic stenosis, end-stage kidney disease requiring hemodialysis, and a history of coronary bypass grafting presented for routine follow-up. B-mode echocardiography showed a severely calcified tricuspid aortic valve with a vibrating calcified nodule and restricted opening, corresponding to severe aortic stenosis. During systole, color Doppler signals were observed around the aortic, pulmonary, and tricuspid valves, mimicking significant pulmonary stenosis and tricuspid regurgitation. However, pulmonary stenosis was ruled out as the pulmonary valve opening was normal. Mild tricuspid regurgitation was confirmed in the apical view.
These cases highlight the diagnostic challenges posed by color Doppler stripes. Recognizing and understanding this artifact are crucial for the accurate diagnosis and management of VHD, ensuring appropriate treatment and patient outcomes.
超声心动图仍然是评估瓣膜性心脏病(VHD)的参考标准成像技术,但像“彩色多普勒条纹”这样的伪影会使诊断变得复杂。这种伪影并未被广泛认识,可能会模拟严重的 VHD,导致潜在的误诊。我们报告了两个彩色多普勒条纹模拟严重 VHD 的病例,强调了在超声心动图评估中需要注意和准确解读。
病例 1:一位 85 岁的患者因疑似严重二尖瓣反流(MR)而被转诊接受二尖瓣手术。评估时,经胸超声心动图(TTE)显示二尖瓣脱垂(P3)和附着在二尖瓣上的高回声、振动结构,提示腱索断裂。彩色多普勒超声心动图显示左心房有强烈的收缩期信号,模拟严重的 MR。经食管超声心动图(TEE)也检测到左心房、左心室和心脏室外的振动结构和彩色多普勒条纹。TEE 上的 PISA 法提示中度 MR,左心室造影显示 Sellers 分级 II 级 MR。该伪影被识别为来自断裂腱索的振动高回声结构引起的彩色多普勒条纹。病例 2:一位 64 岁的患者,患有严重的主动脉瓣狭窄、终末期肾病需要血液透析,以及冠状动脉旁路移植术的病史,来进行常规随访。B 型超声心动图显示严重钙化的三尖瓣主动脉瓣,有一个振动的钙化结节和限制瓣口开放,对应严重的主动脉瓣狭窄。收缩期时,在主动脉瓣、肺动脉瓣和三尖瓣周围观察到彩色多普勒信号,模拟严重的肺动脉瓣狭窄和三尖瓣反流。然而,由于肺动脉瓣开口正常,排除了肺动脉瓣狭窄。在心尖观确认了轻度三尖瓣反流。
这些病例强调了彩色多普勒条纹带来的诊断挑战。认识和理解这种伪影对于准确诊断和管理 VHD 至关重要,确保了适当的治疗和患者的预后。