Monroe Katrina S, Schiehser Dawn M, Parr Aaron W, Simmons Alan N, Hays Weeks Chelsea C, Bailey Barbara A, Shahidi Bahar
School of Physical Therapy, College of Health and Human Services, San Diego State University, 5500 Campanile Dr., San Diego, CA, 92182, USA.
VA San Diego Healthcare System, 3350 La Jolla Village Dr, San Diego, CA 92161; Professor, School of Medicine, Department of Psychiatry, University of California San Diego, 9500 Gilman Dr., San Diego, CA 92093, USA.
medRxiv. 2024 Sep 18:2024.09.16.24313761. doi: 10.1101/2024.09.16.24313761.
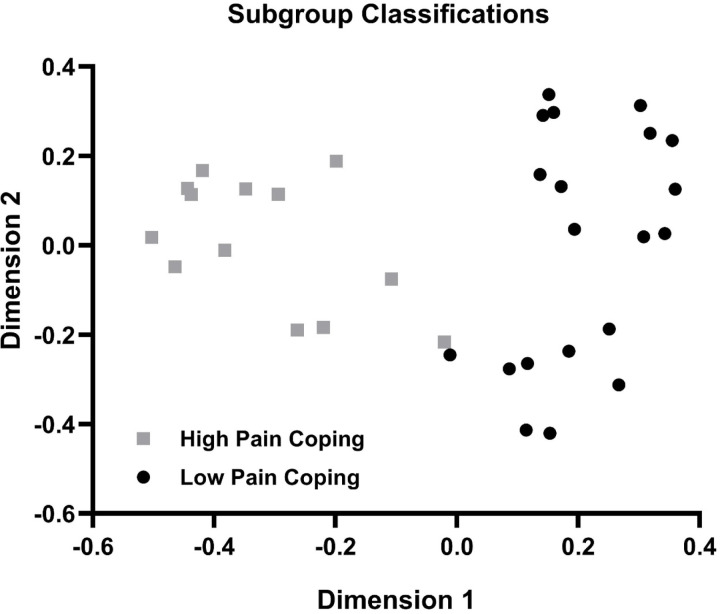
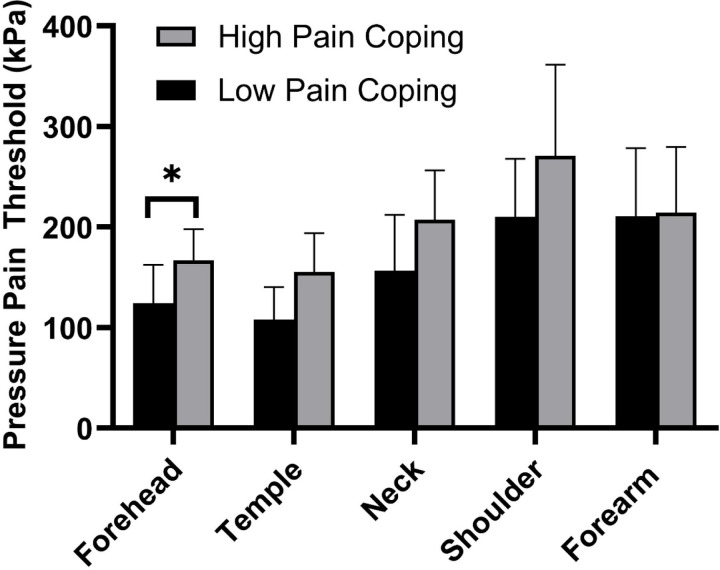
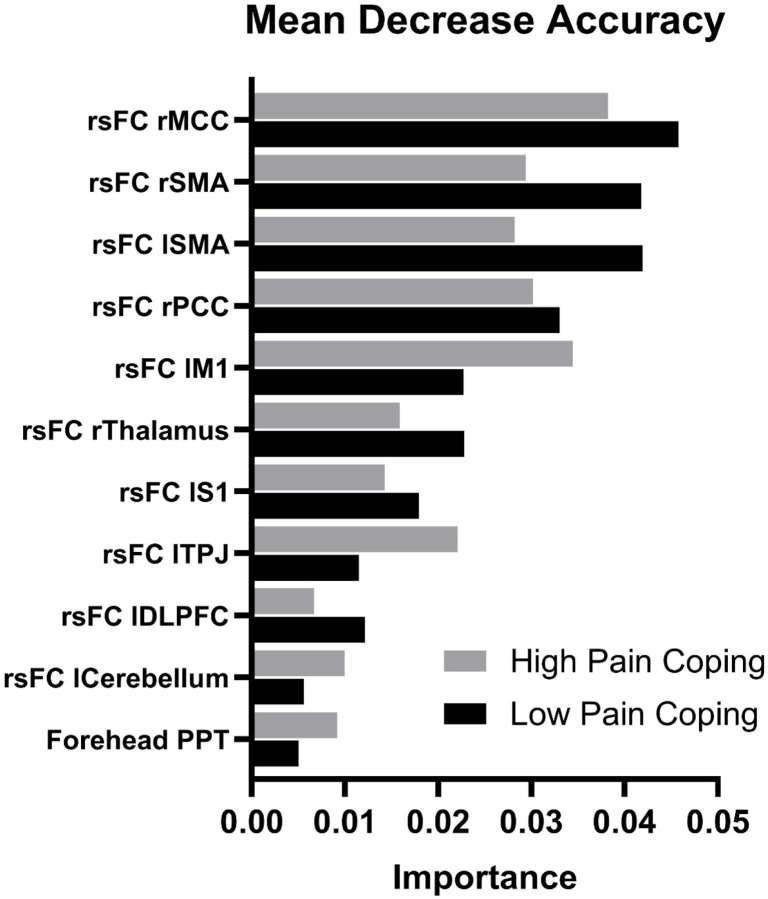
Headache is the most common type of pain following mild traumatic brain injury. Roughly half of those with persistent post-traumatic headache (PPTH) also report neck pain which is associated with greater severity and functional impact of headache. This observational cohort study aimed to identify biological phenotypes to help inform mechanism-based approaches in the management of PPTH with and without concomitant neck pain. Thirty-three military Veterans (mean (SD) = 37±16 years, 29 males) with PPTH completed a clinical assessment, quantitative sensory testing, and magnetic resonance imaging of the brain and cervical spine. Multidimensional phenotyping was performed using a Random Forest analysis and Partitioning Around Medoids (PAM) clustering of input features from three biologic domains: 1) resting state functional connectivity (rsFC) of the periaqueductal gray (PAG), 2) quality and size of cervical muscles, and 3) mechanical pain sensitivity and central modulation of pain. Two subgroups were distinguished by biological features that included forehead pressure pain threshold and rsFC between the PAG and selected nodes within the default mode, salience, and sensorimotor networks. Compared to the High Pain Coping group, the Low Pain Coping group exhibited higher pain-related anxiety (p=0.009), higher pain catastrophizing (p=0.004), lower pain self-efficacy (p=0.010), and greater headache-related disability (p=0.012). Findings suggest that greater functional connectivity of pain modulation networks involving the PAG combined with impairments in craniofacial pain sensitivity, but not cervical muscle health, distinguish a clinically important subgroup of individuals with PPTH who are less able to cope with pain and more severely impacted by headache.
头痛是轻度创伤性脑损伤后最常见的疼痛类型。在患有持续性创伤后头痛(PPTH)的患者中,约有一半还报告有颈部疼痛,这与更严重的头痛程度和功能影响有关。这项观察性队列研究旨在确定生物学表型,以帮助为伴有或不伴有颈部疼痛的PPTH管理中基于机制的方法提供信息。33名患有PPTH的退伍军人(平均(标准差)=37±16岁,29名男性)完成了临床评估、定量感觉测试以及脑部和颈椎的磁共振成像。使用随机森林分析和围绕中心点划分法(PAM)聚类对来自三个生物学领域的输入特征进行多维度表型分析:1)导水管周围灰质(PAG)的静息态功能连接(rsFC),2)颈部肌肉的质量和大小,3)机械性疼痛敏感性和疼痛的中枢调制。通过生物学特征区分出两个亚组,这些特征包括前额压痛阈值以及PAG与默认模式、突显网络和感觉运动网络内选定节点之间的rsFC。与高疼痛应对组相比,低疼痛应对组表现出更高的疼痛相关焦虑(p=0.009)、更高的疼痛灾难化(p=0.004)、更低的疼痛自我效能感(p=0.010)以及更大的头痛相关残疾(p=0.012)。研究结果表明,涉及PAG的疼痛调制网络的功能连接增强,同时伴有颅面部疼痛敏感性受损,但不包括颈部肌肉健康状况,可区分出一个临床上重要的PPTH患者亚组,这些患者应对疼痛的能力较差,且受头痛影响更严重。