Iftimovici Anton, Krebs Emma, Dalfin William, Legrand Adrien, Scoriels Linda, Martinez Gilles, Bendjemaa Narjes, Duchesnay Edouard, Chaumette Boris, Krebs Marie-Odile
Université Paris Cité, Institute of Psychiatry and Neuroscience of Paris (IPNP), INSERM U1266, Paris, France.
Institut de Psychiatrie, CNRS GDR 3557, Paris, France.
Psychol Med. 2024 Oct 15;54(13):1-12. doi: 10.1017/S0033291724001776.
Treatment resistance is a major challenge in psychiatric disorders. Early detection of potential future resistance would improve prognosis by reducing the delay to appropriate treatment adjustment and recovery. Here, we sought to determine whether neurodevelopmental markers can predict therapeutic response.
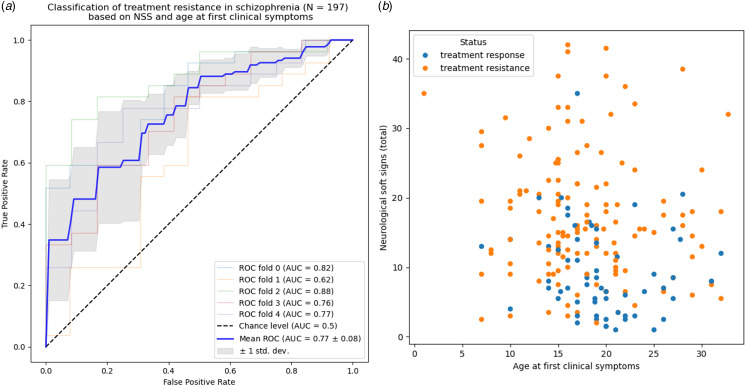
Healthy controls ( = 236), patients with schizophrenia ( = 280) or bipolar disorder ( = 78) with a known therapeutic outcome, were retrospectively included. Age, sex, education, early developmental abnormalities (obstetric complications, height, weight, and head circumference at birth, hyperactivity, dyslexia, epilepsy, enuresis, encopresis), neurological soft signs (NSS), and ages at first subjective impairment, clinical symptoms, treatment, and hospitalization, were recorded. A supervised algorithm leveraged NSS and age at first clinical signs to classify between resistance and response in schizophrenia.
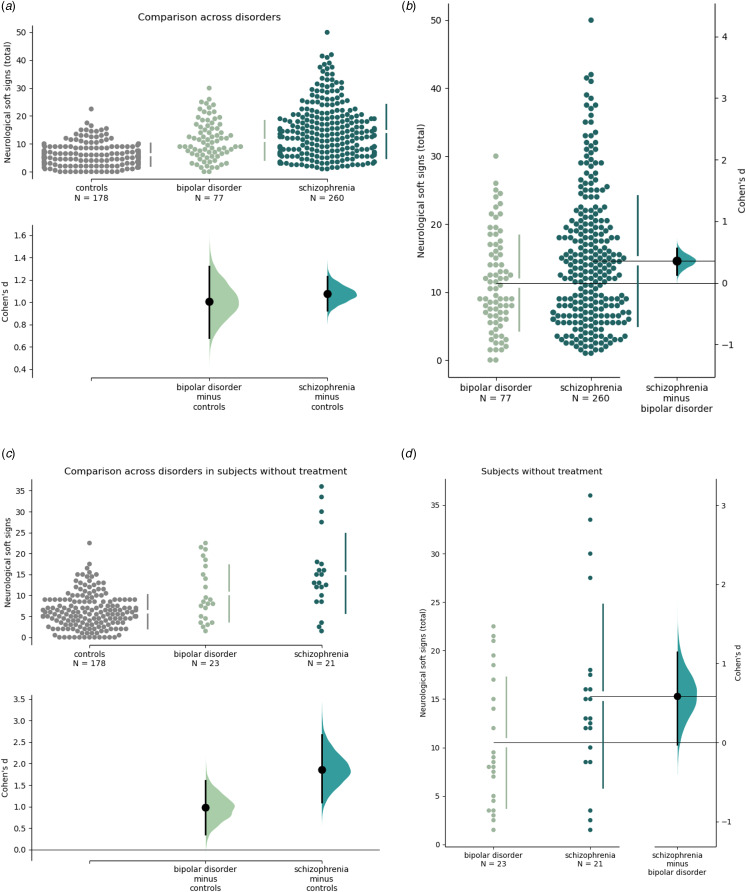
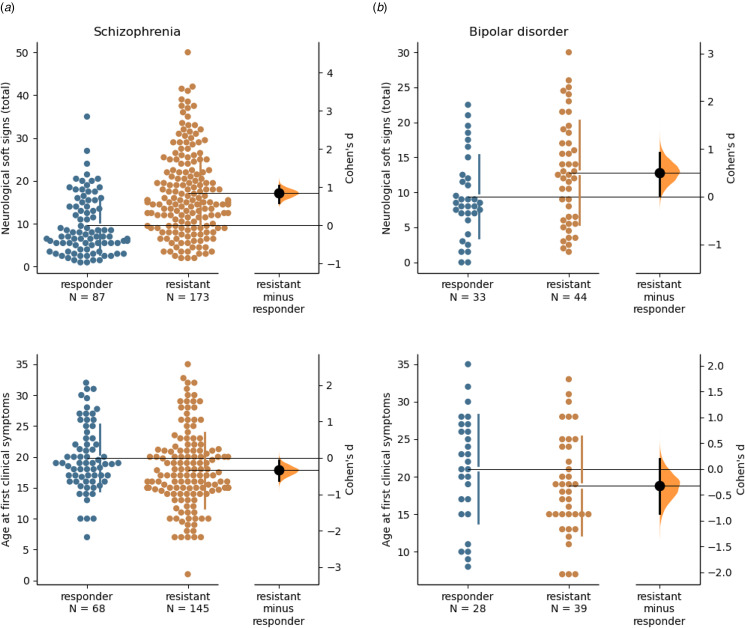
Developmental abnormalities were more frequent in schizophrenia and bipolar disorder than in controls. NSS significantly differed between controls, responsive, and resistant participants with schizophrenia (5.5 ± 3.0, 7.0 ± 4.0, 15.0 ± 6.0 respectively, = 3 × 10) and bipolar disorder (5.5 ± 3.0, 8.3 ± 3.0, 12.5 ± 6.0 respectively, < 1 × 10). In schizophrenia, but not in bipolar disorder, age at first subjective impairment was three years lower, and age at first clinical signs two years lower, in resistant than responsive subjects ( = 2 × 10 and = 9 × 10, respectively). Age at first clinical signs and NSS accurately predicted treatment response in schizophrenia (area-under-curve: 77 ± 8%, = 1 × 10).
Neurodevelopmental features such as NSS and age of clinical onset provide a means to identify patients who may require rapid treatment adaptation.
治疗抵抗是精神疾病的一项重大挑战。早期发现潜在的未来抵抗情况,可通过减少适当治疗调整和康复的延迟来改善预后。在此,我们试图确定神经发育标志物是否能够预测治疗反应。
回顾性纳入了健康对照者(n = 236)、已知治疗结果的精神分裂症患者(n = 280)或双相情感障碍患者(n = 78)。记录年龄、性别、教育程度、早期发育异常情况(产科并发症、出生时的身高、体重和头围、多动、阅读障碍、癫痫、遗尿、遗粪)、神经软体征(NSS)以及首次主观功能损害、临床症状、治疗和住院的年龄。一种监督算法利用NSS和首次临床体征出现时的年龄,对精神分裂症患者的抵抗和反应进行分类。
精神分裂症和双相情感障碍患者的发育异常情况比对照者更常见。对照者、有反应的精神分裂症患者和抵抗的精神分裂症患者之间的NSS存在显著差异(分别为5.5±3.0、7.0±4.0、15.0±6.0,P = 3×10),双相情感障碍患者之间也存在显著差异(分别为5.5±3.0、8.3±3.0、12.5±6.0,P < 1×10)。在精神分裂症中,而非双相情感障碍中,抵抗患者的首次主观功能损害年龄比有反应患者低3岁,首次临床体征出现时的年龄低2岁(分别为P = 2×10和P = 9×10)。首次临床体征出现时的年龄和NSS准确预测了精神分裂症的治疗反应(曲线下面积:77±8%,P = 1×10)。
诸如NSS和临床起病年龄等神经发育特征提供了一种识别可能需要快速调整治疗的患者的方法。