Department of Obstetrics and Gynecology, Osmaniye State Hospital, Selimiye, Bölge Trafik Yanı, Musa Şahin Blv, 80000, Osmaniye, Merkez, Turkey.
Department of Gynecological Oncology, Nyala Sudan Turkish Training and Research Hospital, Nyala, South Darfur, Sudan.
BMC Womens Health. 2024 Oct 21;24(1):567. doi: 10.1186/s12905-024-03406-3.
This study aims to examine cases identified with endometrial polyp and carcinoma originating from polyps in patients presenting with gynaecological problems, and to highlight the significance of risk factors contributing to malignancy.
The study comprised 203 patients who visited our clinic between January 2019 and 2024 with various gynaecological problems and were identified with endometrial polyps after a clinical, radiographic, and laboratory assessment. We retrospectively analysed data from 191 benign endometrial polyps and hyperplasia without atypia and 12 patients with endometrial polyps and underlying endometrial hyperplasia with atypia and/or endometrial carcinoma, diagnosed histopathologically after hysteroscopic resection, retrieved from our hospital's electronic archive system. Two hundred three participants were tested in the study, with 191 classifieds with benign tumours and 12 diagnosed with malignant tumours and atypical endometrial hyperplasia (premalignant). Cases were chosen according on consistent criteria for age, BMI, gravida, parity, abortion, educational level, smoking habits, operation history, and co-morbidities. After determining the sample size for the malignant group, patients from the control group were selected to be included in the study. Initially, patients with similar age and BMI distributions were included into the study. Next, the cases were analysed for similarities in gravida, parity, and abortion parameters, and those that matched were chosen. Following this step, the educational status was compared for resemblance, and examples with matching educational status were chosen. Consequently, the study covered a total of 34 patients, with 12 identified with malignant tumours and atypical endometrial hyperplasia (premalignant) and 22 with benign tumours. Two groups of cases were diagnosed with endometrial polyp, and risk factors that may cause the development of endometrial polyp and underlying carcinoma: age, gravida, parity, abortion, education level, smoking, previous operation history, comorbidity, gynaecological complaints, fasting blood sugar, CRP values, haemoglobin, and haematocrit were evaluated in terms of endometrial polyp sizes, endometrial thickness level, and endometrial polyp localization. By examining the pathological risk factors of these cases, particularly during the premenopausal period, the goal is to predict endometrial cancer, the most prevalent gynaecological cancer in women, along with its antecedents, and implement preventive measures proactively.
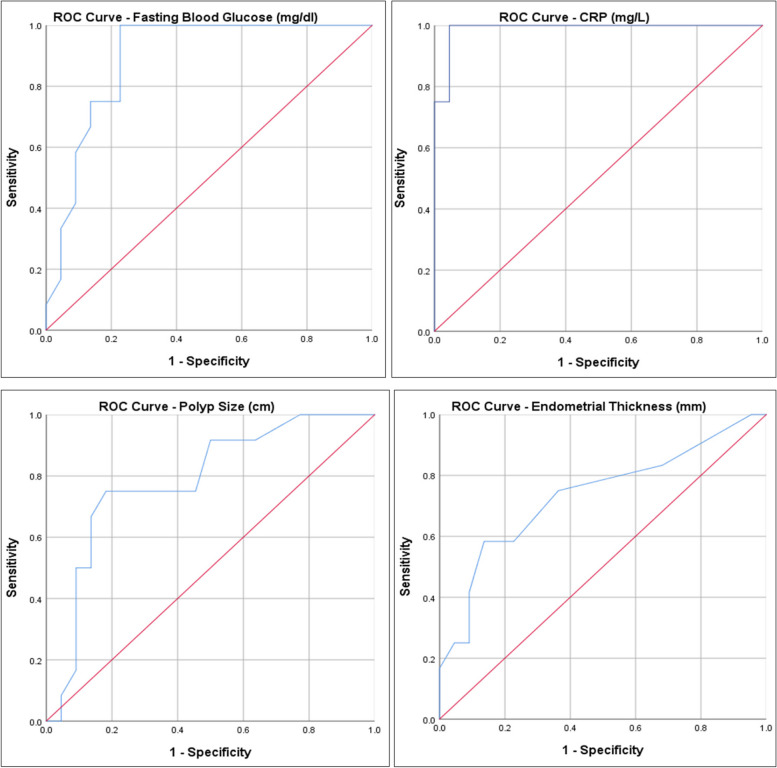
Age, BMI, gravida, parity, number of abortions, educational status, smoking status, operation history, co-morbidity, and complaint variables did not exhibit a statistically significant difference between the groups (p > 0.05). It was revealed that the FBG level, CRP level, Polyp length and Endometrial thickness level of the malignant group were statistically significantly higher than the benign group (p < 0.01) (p < 0.05). Upon analysing the FBG distribution among groups, it is noted that the ODDS ratio is 10.20 for FBG values of 122.5 and above (95% CI: 1.97 - 52.78). Upon analysing the CRP distribution by groups, it is noted that the ODDS ratio is 231 for CRP values of 9.7 and above (95% CI: 13.15 - 4058.67). Upon analysing the distribution of Polyp length based on groups, it was determined that the ODDS ratio is 13.5 for Polyp lengths of 2.25 and above (95% CI: 2.47 - 73.71). Upon analysing the distribution of EM thickness based on groups, it is shown that the ODDS ratio is 5.25 for EM thicknesses of 11 and above (95% CI: 1.09 - 25.21).
Endometrial polyps are common benign growths that are typically not seen as cancer precursors but may be linked to cancer in people with advanced age. It is vital to remember that in cases of endometrial polyps, variables such as increasing polyp length, endometrial thickness, fasting glucose level, and elevated CRP levels are significant risk factors for the development of cancer associated with polyps.
本研究旨在检查因妇科问题就诊并经临床、影像学和实验室评估后被诊断为子宫内膜息肉的患者中源自息肉的子宫内膜息肉和癌病例,并强调导致恶性肿瘤的风险因素的重要性。
本研究纳入了 203 名 2019 年 1 月至 2024 年期间因各种妇科问题就诊且经临床、影像学和实验室评估后被诊断为子宫内膜息肉的患者。我们回顾性分析了从我们医院电子档案系统中检索到的 191 例良性子宫内膜息肉和非典型增生无增生以及 12 例子宫内膜息肉和潜在子宫内膜增生伴不典型增生和/或子宫内膜癌的患者的数据,这些患者经宫腔镜切除术后组织病理学诊断。203 名参与者在研究中进行了测试,其中 191 例为良性肿瘤患者,12 例为恶性肿瘤和不典型子宫内膜增生(癌前病变)患者。根据年龄、BMI、孕次、产次、流产、教育水平、吸烟习惯、手术史和合并症等一致标准选择病例。确定恶性组的样本量后,从对照组中选择患者纳入研究。首先,将具有相似年龄和 BMI 分布的患者纳入研究。接下来,分析了孕次、产次和流产参数的相似性,并选择了匹配的病例。在这一步之后,比较了教育状况的相似性,并选择了具有匹配教育状况的例子。因此,该研究共包括 34 例患者,其中 12 例为恶性肿瘤和不典型子宫内膜增生(癌前病变)患者,22 例为良性肿瘤患者。两组患者均被诊断为子宫内膜息肉,并评估了可能导致子宫内膜息肉和潜在癌发展的风险因素:年龄、孕次、产次、流产、教育水平、吸烟、既往手术史、合并症、妇科主诉、空腹血糖、CRP 值、血红蛋白和血细胞比容与子宫内膜息肉大小、子宫内膜厚度水平和子宫内膜息肉定位有关。通过检查这些病例的病理危险因素,特别是在绝经前期间,旨在预测最常见的妇科癌症——子宫内膜癌及其前身,并主动采取预防措施。
年龄、BMI、孕次、产次、流产次数、教育水平、吸烟状况、手术史、合并症和主诉变量在组间没有统计学差异(p>0.05)。结果表明,恶性组的 FBG 水平、CRP 水平、息肉长度和子宫内膜厚度水平均显著高于良性组(p<0.01)(p<0.05)。在分析组间 FBG 分布时,注意到 FBG 值为 122.5 及以上的 ODDS 比值为 10.20(95%CI:1.97-52.78)。在分析 CRP 分布时,注意到 CRP 值为 9.7 及以上的 ODDS 比值为 231(95%CI:13.15-4058.67)。在分析基于组的息肉长度分布时,确定息肉长度为 2.25 及以上的 ODDS 比值为 13.5(95%CI:2.47-73.71)。在分析基于组的 EM 厚度分布时,表明 EM 厚度为 11 及以上的 ODDS 比值为 5.25(95%CI:1.09-25.21)。
子宫内膜息肉是常见的良性生长物,通常不被视为癌症前体,但在年龄较大的人群中可能与癌症有关。重要的是要记住,在子宫内膜息肉的情况下,息肉长度、子宫内膜厚度、空腹血糖水平和 CRP 水平升高等变量是与息肉相关癌症的重要危险因素。