Morioka Tsubasa, Kato Shingo, Onoma Ayano, Izumi Toshiharu, Sakano Tomokazu, Ishikawa Eiji, Sawamura Shungo, Yasuda Naofumi, Nagase Hiroaki, Utsunomiya Daisuke
Department of Radiology, Yokohama City University Hospital, Yokohama 236-0004, Kanagawa, Japan.
Department of Diagnostic Radiology, Yokohama City University Graduate School of Medicine, Yokohama 236-0004, Kanagawa, Japan.
J Cardiovasc Dev Dis. 2024 Oct 2;11(10):304. doi: 10.3390/jcdd11100304.
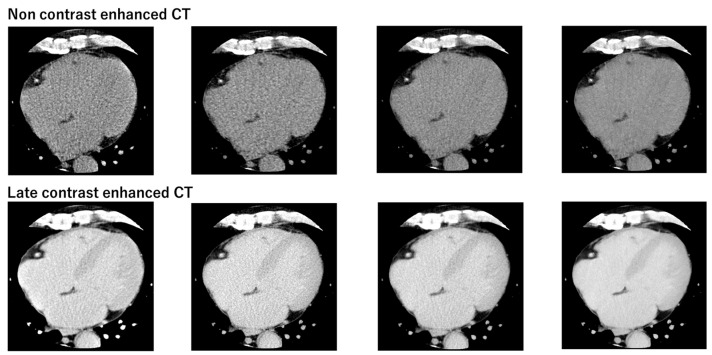
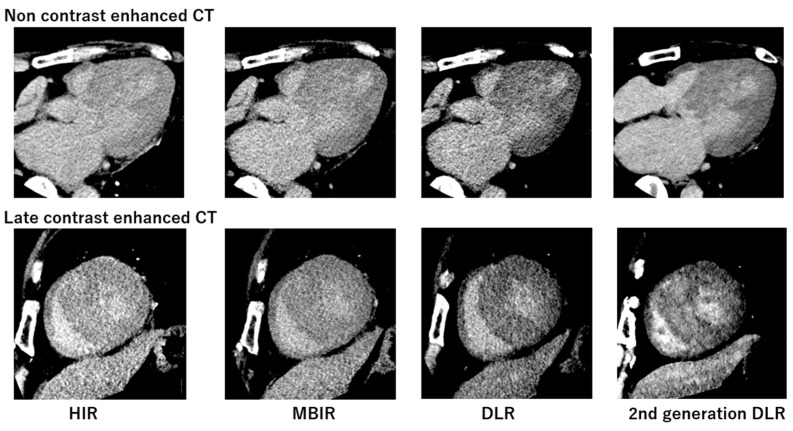
The utility of synthetic ECV, which does not require hematocrit values, has been reported; however, high-quality CT images are essential for accurate quantification. Second-generation Deep Learning Reconstruction (DLR) enables low-noise and high-resolution cardiac CT images. The aim of this study is to compare the differences among four reconstruction methods (hybrid iterative reconstruction (HIR), model-based iterative reconstruction (MBIR), DLR, and second-generation DLR) in the quantification of synthetic ECV.
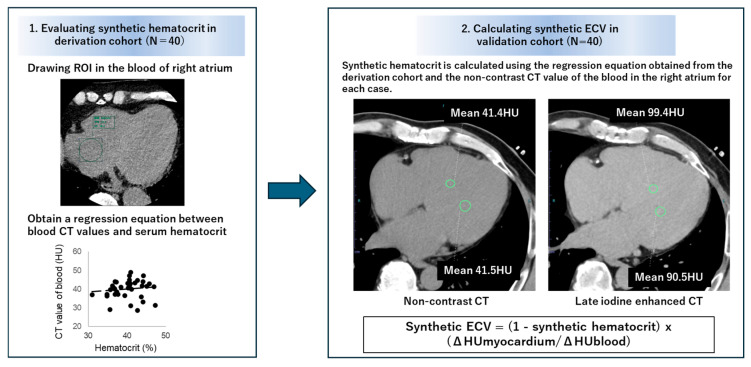
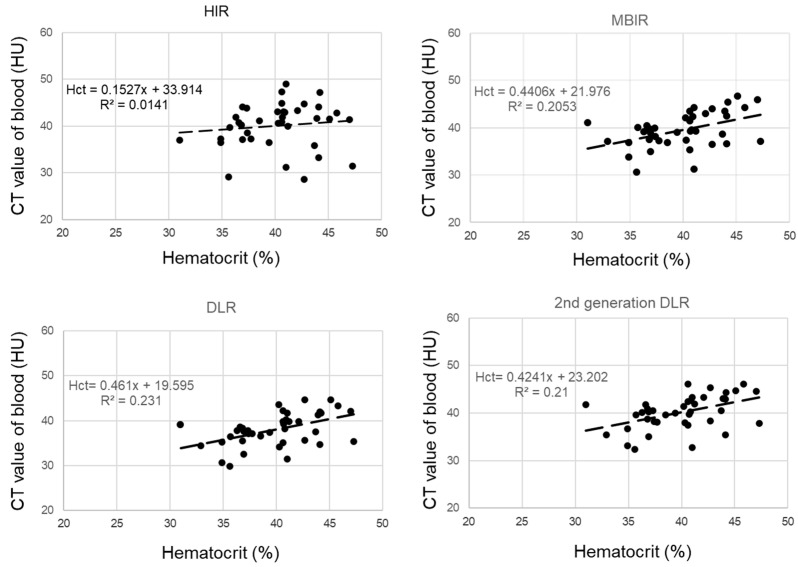
We retrospectively analyzed 80 patients who underwent cardiac CT scans, including late contrast-enhanced CT (derivation cohort: = 40, age 71 ± 12 years, 24 males; validation cohort: = 40, age 67 ± 11 years, 25 males). In the derivation cohort, a linear regression analysis was performed between the hematocrit values from blood tests and the CT values of the right atrial blood pool on non-contrast CT. In the validation cohort, synthetic hematocrit values were calculated using the linear regression equation and the right atrial CT values from non-contrast CT. The correlation and mean difference between synthetic ECV and laboratory ECV calculated from actual blood tests were assessed.
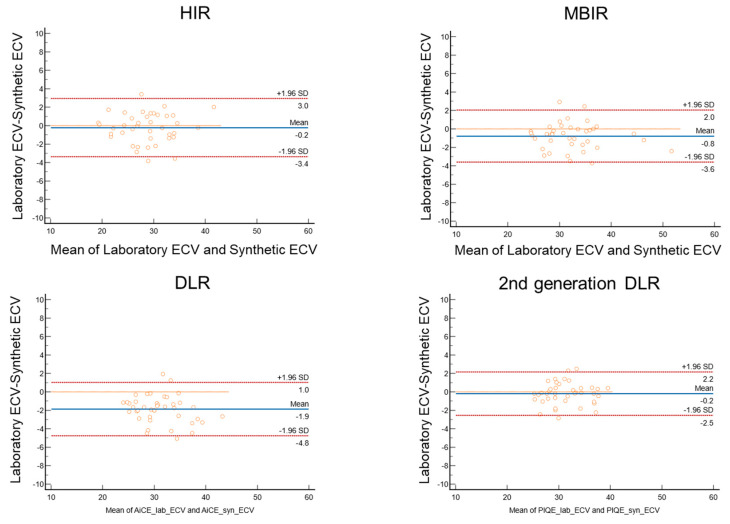
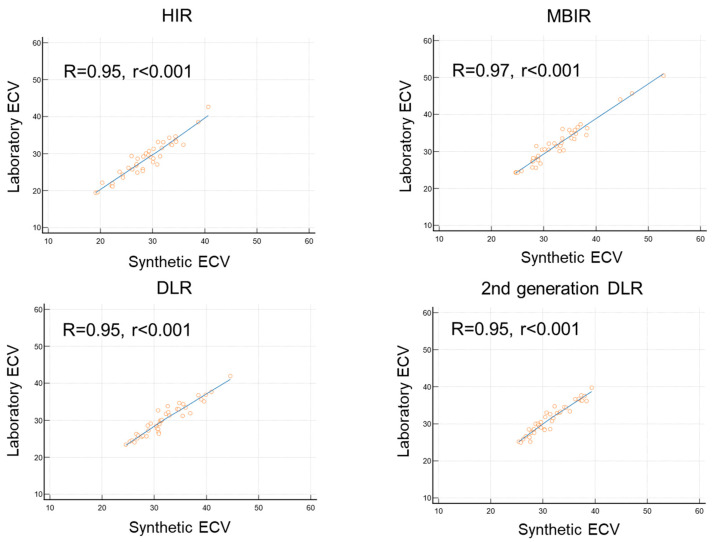
Synthetic ECV and laboratory ECV showed a high correlation across all four reconstruction methods (R ≥ 0.95, < 0.001). The bias and limit of agreement (LOA) in the Bland-Altman plot were lowest with the second-generation DLR (hybrid IR: bias = -0.21, LOA: 3.16; MBIR: bias = -0.79, LOA: 2.81; DLR: bias = -1.87, LOA: 2.90; second-generation DLR: bias = -0.20, LOA: 2.35).
Synthetic ECV using second-generation DLR demonstrated the lowest bias and LOA compared to laboratory ECV among the four reconstruction methods, suggesting that second-generation DLR enables more accurate quantification.
已报道了无需血细胞比容值的合成细胞外容积(ECV)的效用;然而,高质量的CT图像对于准确量化至关重要。第二代深度学习重建(DLR)可实现低噪声和高分辨率的心脏CT图像。本研究的目的是比较四种重建方法(混合迭代重建(HIR)、基于模型的迭代重建(MBIR)、DLR和第二代DLR)在合成ECV量化方面的差异。
我们回顾性分析了80例行心脏CT扫描的患者,包括延迟对比增强CT(推导队列:n = 40,年龄71±12岁,男性24例;验证队列:n = 40,年龄67±11岁,男性25例)。在推导队列中,对血液检测的血细胞比容值与非增强CT上右心房血池的CT值进行线性回归分析。在验证队列中,使用线性回归方程和非增强CT上的右心房CT值计算合成血细胞比容值。评估合成ECV与通过实际血液检测计算得到的实验室ECV之间的相关性和平均差异。
在所有四种重建方法中,合成ECV与实验室ECV均显示出高度相关性(R≥0.95,P<0.001)。第二代DLR在Bland-Altman图中的偏差和一致性界限(LOA)最低(混合IR:偏差=-0.21,LOA:3.16;MBIR:偏差=-0.79,LOA:2.