Steinke Philipp, Schupp Tobias, Kuhn Lasse, Abumayyaleh Mohammad, Weidner Kathrin, Bertsch Thomas, Schmitt Alexander, Jannesari Mahboubeh, Siegel Fabian, Duerschmied Daniel, Behnes Michael, Akin Ibrahim
Department of Cardiology, Angiology, Haemostaseology and Medical Intensive Care, University Medical Centre Mannheim, Medical Faculty Mannheim, Heidelberg University, 68167 Mannheim, Germany.
Institute of Clinical Chemistry, Laboratory Medicine and Transfusion Medicine, Nuremberg General Hospital, Paracelsus Medical University, 90419 Nuremberg, Germany.
J Clin Med. 2024 Oct 12;13(20):6088. doi: 10.3390/jcm13206088.
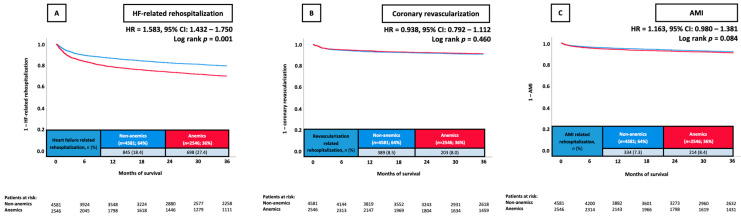
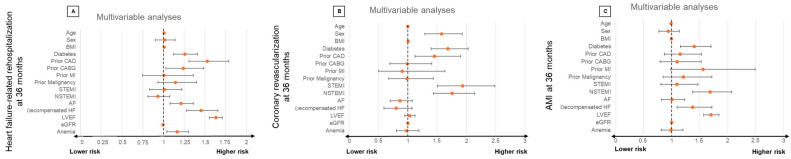
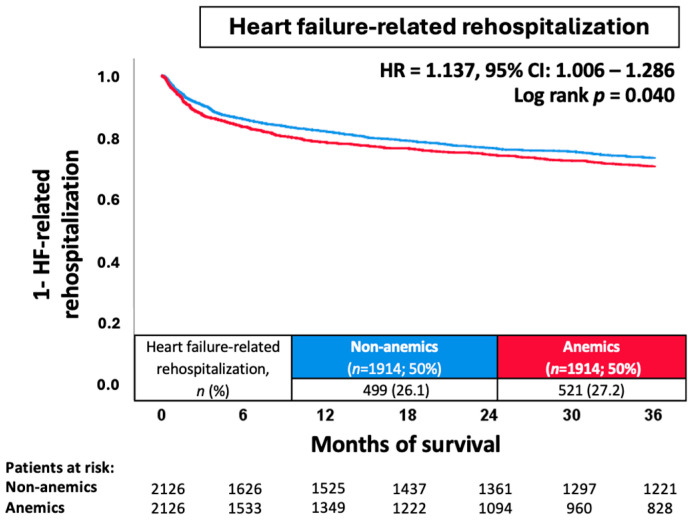
: This study investigates the prevalence and prognostic impact of concomitant anemia in unselected patients undergoing invasive coronary angiography (CA). The spectrum of patients undergoing CA has significantly changed during the past decades, related to ongoing demographic changes and improved treatment strategies for patients with cardiovascular disease. : Consecutive patients undergoing invasive CA from 2016 to 2022 were retrospectively included at one institution. Patients with anemia (i.e., hemoglobin < 13.0 g/dL for males and <12.0 g/dL for females) were compared with patients without anemia (i.e., nonanemics). The primary endpoint was rehospitalization for heart failure (HF) at 36 months. Secondary endpoints comprised the risk of rehospitalization for acute myocardial infarction (AMI) and coronary revascularization. Statistical analyses included Kaplan-Meier, multivariable Cox proportional regression analyses, and propensity score matching. : From 2016 to 2022, 7645 patients undergoing CA were included with a median hemoglobin level of 13.2 g/dL. Anemics had a higher prevalence of coronary artery disease (CAD) (76.3% vs. 74.8%; = 0.001), alongside an increased need for percutaneous coronary intervention (PCI) (45.3% vs. 41.5%; = 0.001). At 36 months, the risk of rehospitalization for HF was higher in anemic patients (27.4% vs. 18.4%; = 0.001; HR = 1.583; 95% CI 1.432-1.750; = 0.001), which was still evident after multivariable adjustment (HR = 1.164; 95% CI 1.039-1.304; = 0.009) and propensity score matching (HR = 1.137; 95% CI 1.006-1.286; = 0.040). However, neither the risk of AMI (8.4% vs. 7.4%, = 0.091) nor the risk of coronary revascularization at 36 months (8.0% vs. 8.5%, = 0.447) was higher in anemic compared with nonanemic patients. : In consecutive patients undergoing CA, concomitant anemia was independently associated with an increased risk of rehospitalization for HF, but not AMI or coronary revascularization. Patients with LVEF ≥ 35% and multivessel disease were especially susceptible to anemia-induced HF-related rehospitalization.
本研究调查了接受有创冠状动脉造影(CA)的未经选择的患者中合并贫血的患病率及其预后影响。在过去几十年中,由于人口结构的不断变化以及心血管疾病患者治疗策略的改进,接受CA的患者群体已发生显著变化。
对2016年至2022年在一家机构接受有创CA的连续患者进行了回顾性纳入。将贫血患者(即男性血红蛋白<13.0 g/dL,女性血红蛋白<12.0 g/dL)与非贫血患者(即非贫血者)进行比较。主要终点是36个月时因心力衰竭(HF)再次住院。次要终点包括急性心肌梗死(AMI)再次住院和冠状动脉血运重建的风险。统计分析包括Kaplan-Meier分析、多变量Cox比例回归分析和倾向得分匹配。
2016年至2022年,共纳入7645例接受CA的患者,血红蛋白水平中位数为13.2 g/dL。贫血患者的冠状动脉疾病(CAD)患病率更高(76.3%对74.8%;P = 0.001),同时接受经皮冠状动脉介入治疗(PCI)的需求也增加(45.3%对41.5%;P = 0.001)。在36个月时,贫血患者因HF再次住院的风险更高(27.4%对18.4%;P = 0.001;HR = 1.583;95%CI 1.432 - 1.750;P = 0.001),在多变量调整后(HR = 1.164;95%CI 1.039 - 1.304;P = 0.009)和倾向得分匹配后(HR = 1.137;95%CI 1.006 - 1.286;P = 0.040)仍然明显。然而,与非贫血患者相比,贫血患者的AMI风险(8.4%对7.4%,P = 0.091)和36个月时的冠状动脉血运重建风险(8.0%对8.5%,P = 0.447)均未更高。
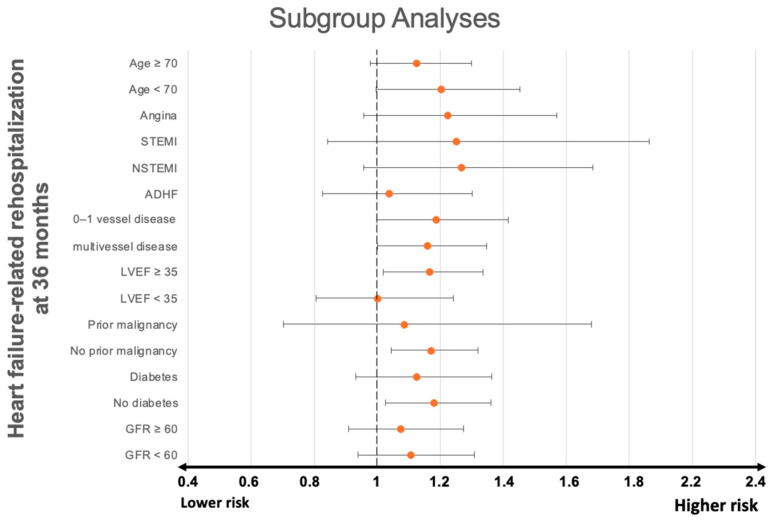
在接受CA的连续患者中,合并贫血与HF再次住院风险增加独立相关,但与AMI或冠状动脉血运重建无关。左心室射血分数(LVEF)≥35%且患有多支血管病变的患者尤其容易因贫血导致与HF相关的再次住院。