Looka Andrew, Qualls David A, Matthews Daniel, Redd Robert A, Sakellis Christopher, Duffy Caitlyn, Dela Cruz Jamie, Saucier Anna, Armand Philippe, Crombie Jennifer L, Fisher David C, Jacobsen Eric D, Kim Austin I, LaCasce Ann S, Merryman Reid W, Parry Erin M, Jacobson Caron A
Division of Lymphoma, Department of Medicine, Dana-Farber Cancer Institute, Boston, MA.
Department of Data Science, Dana-Farber Cancer Institute, Boston, MA.
Blood Adv. 2025 Feb 11;9(3):455-462. doi: 10.1182/bloodadvances.2024012992.
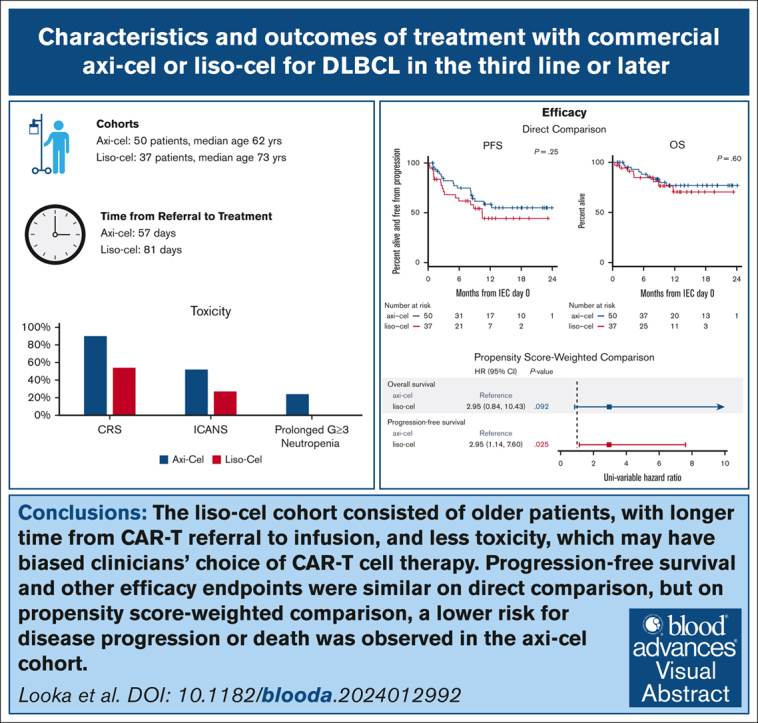
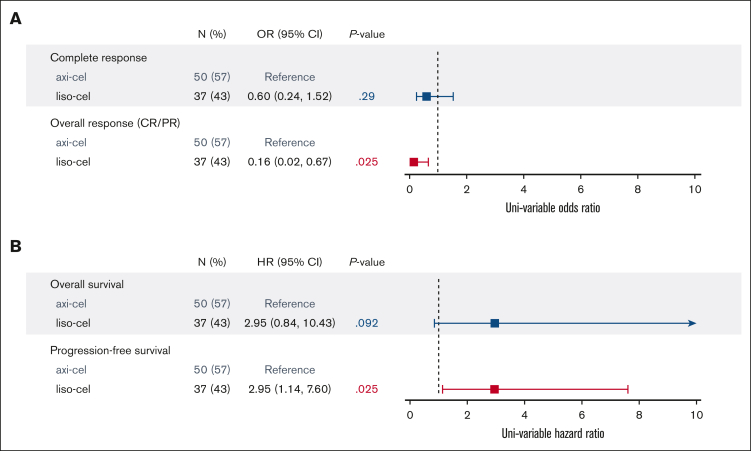
Lisocabtagene maraleucel (liso-cel) and axicabtagene ciloleucel (axi-cel) are anti-CD19 chimeric antigen receptor (CAR) T-cell therapies approved for relapsed and refractory large B-cell lymphoma (LBCL); however, there is currently no published data on liso-cel outside of clinical trials nor any data comparing these therapies. In this retrospective analysis, we reviewed patients with LBCL receiving liso-cel or axi-cel at a single institution in the third-line setting. From June 2021 to September 2022, a total of 50 patients received axi-cel and 37 liso-cel. Baseline patient characteristics were similar, aside from older age in liso-cel recipients. The median time from leukapheresis to CAR T-cell infusion was significantly longer for liso-cel (41 days) than axi-cel (30 days). Complete response rates were not significantly different between axi-cel (72%) and liso-cel (62%). At a median follow-up of 11 months, progression-free survival (PFS) was not significantly different between axi-cel and liso-cel cohorts, with 12-month PFS of 59% and 44%, respectively. However, on a propensity score analysis, an inferior PFS was observed with liso-cel (hazard ratio, 2.95; 95% confidence interval , 1.14-7.60). The rates of cytokine release syndrome, immune effector cell-associated neurotoxicity syndrome, and prolonged neutropenia were higher with axi-cel than liso-cel. Overall, direct comparison of axi-cel and liso-cel cohorts shows similar key outcomes including response rate and PFS, but prolonged wait times for liso-cel may have resulted in biased selection of patients with more favorable characteristics for liso-cel. When accounting for these higher-risk characteristics, an inferior PFS is observed with liso-cel compared with axi-cel. These findings warrant further evaluation in a multicenter setting.
利妥昔单抗(liso-cel)和阿基仑赛(axi-cel)是两种抗CD19嵌合抗原受体(CAR)T细胞疗法,已被批准用于复发难治性大B细胞淋巴瘤(LBCL);然而,目前除了临床试验之外,没有关于利妥昔单抗的已发表数据,也没有比较这两种疗法的数据。在这项回顾性分析中,我们回顾了在三线治疗环境下于单一机构接受利妥昔单抗或阿基仑赛治疗的LBCL患者。从2021年6月至2022年9月,共有50例患者接受了阿基仑赛治疗,37例接受了利妥昔单抗治疗。除了接受利妥昔单抗治疗的患者年龄较大外,患者的基线特征相似。利妥昔单抗从白细胞分离术到CAR T细胞输注的中位时间(41天)显著长于阿基仑赛(30天)。阿基仑赛(72%)和利妥昔单抗(62%)的完全缓解率没有显著差异。在中位随访11个月时,阿基仑赛和利妥昔单抗队列的无进展生存期(PFS)没有显著差异,12个月PFS分别为59%和44%。然而,在倾向评分分析中,观察到利妥昔单抗的PFS较差(风险比,2.95;95%置信区间,1.14 - 7.60)。阿基仑赛的细胞因子释放综合征、免疫效应细胞相关神经毒性综合征和长期中性粒细胞减少的发生率高于利妥昔单抗。总体而言,阿基仑赛和利妥昔单抗队列的直接比较显示出相似的关键结果,包括缓解率和PFS,但利妥昔单抗较长的等待时间可能导致对利妥昔单抗选择了特征更有利的患者,从而产生偏差。在考虑这些高风险特征时,与阿基仑赛相比,利妥昔单抗的PFS较差。这些发现值得在多中心环境中进一步评估。