Faculty of Rehabilitation, University of Physical Education in Kraków, Kraków, Poland.
Kleijnen Systematic Reviews Ltd, York, UK.
Syst Rev. 2024 Nov 29;13(1):296. doi: 10.1186/s13643-024-02719-6.
This update of a systematic review evaluates the effectiveness of spinal manipulations as a treatment for migraine headaches.
Spinal manipulation therapy (SMT) is sometimes used to treat migraine headaches; however, the biological plausibility and safety of SMT have repeatedly been questioned.
Amed, Embase, MEDLINE, CINAHL, Mantis, Index to Chiropractic Literature, and Cochrane Central were searched from inception to September 2023. Randomized clinical trials (RCTs) investigating spinal manipulations (performed by various healthcare professionals including physiotherapists, osteopaths, and chiropractors) for treating migraine headaches in human subjects were considered. Other types of manipulative therapy, i.e., cranial, visceral, and soft tissue were excluded. The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was used to evaluate the certainty of evidence.
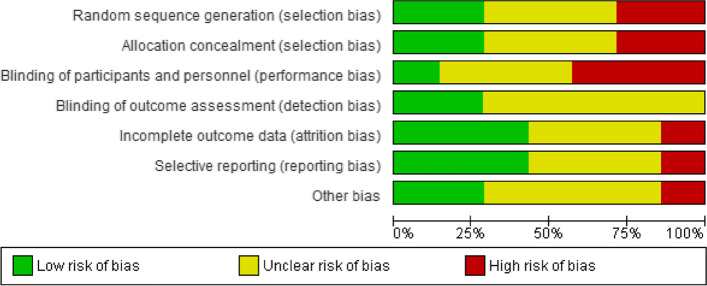
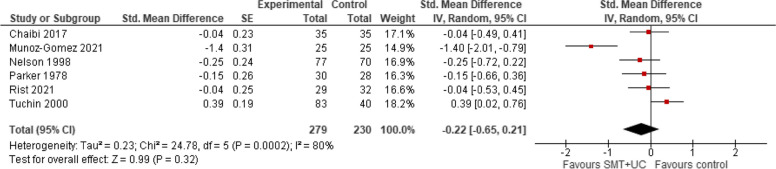
Three more RCTs were published since our first review; amounting to a total of 6 studies with 645 migraineurs meeting the inclusion criteria. Meta-analysis of six trials showed that, compared with various controls (placebo, drug therapy, usual care), SMT (with or without usual care) has no effect on migraine intensity/severity measured with a range of instruments (standardized mean difference [SMD] - 0.22, 95% confidence intervals [CI] - 0.65 to 0.21, very low certainty evidence), migraine duration (SMD - 0.10; 95% CI - 0.33 to 0.12, 4 trials, low certainty evidence), or emotional quality of life (SMD - 14.47; 95% CI - 31.59 to 2.66, 2 trials, low certainty evidence) at post-intervention. A meta-analysis of two trials showed that compared with various controls, SMT (with or without usual care) increased the risk of AEs (risk ratio [RR] 2.06; 95% CI 1.24 to 3.41, numbers needed to harm = 6; very low certainty evidence). The main reasons for downgrading the evidence were study limitations (studies judged to be at an unclear or high risk of bias), inconsistency (for pain intensity/severity), imprecision (small sizes and wide confidence intervals around effect estimates) and indirectness (methodological and clinical heterogeneity of populations, interventions, and comparators).
The effectiveness of SMT for the treatment of migraines remains unproven. Future, larger, more rigorous, and independently conducted studies might reduce the existing uncertainties.
本次系统评价更新旨在评估脊柱推拿作为偏头痛治疗方法的有效性。
脊柱推拿疗法(SMT)有时用于治疗偏头痛,但 SMT 的生物学合理性和安全性一再受到质疑。
自成立以来,检索了 Amed、Embase、MEDLINE、CINAHL、Mantis、脊椎按摩文献索引和 Cochrane 中心,以寻找针对人类偏头痛患者的脊柱推拿(由各种医疗保健专业人员进行,包括物理治疗师、整骨医生和脊医)的随机临床试验(RCT)。排除了其他类型的推拿疗法,即颅、内脏和软组织推拿。使用推荐评估、制定与评价(GRADE)方法评估证据的确定性。
自我们首次审查以来,又有三项 RCT 发表,总共纳入了 6 项研究,共有 645 名偏头痛患者符合纳入标准。六项试验的荟萃分析表明,与各种对照(安慰剂、药物治疗、常规护理)相比,SMT(单独或联合常规护理)对使用各种仪器测量的偏头痛强度/严重程度(标准化均数差[SMD] -0.22,95%置信区间[CI] -0.65 至 0.21,极低确定性证据)、偏头痛持续时间(SMD -0.10;95%CI -0.33 至 0.12,4 项试验,低确定性证据)或情绪生活质量(SMD -14.47;95%CI -31.59 至 2.66,2 项试验,低确定性证据)均无影响。两项试验的荟萃分析表明,与各种对照相比,SMT(单独或联合常规护理)增加了不良反应的风险(风险比[RR] 2.06;95%CI 1.24 至 3.41,需要治疗的人数=6;极低确定性证据)。降低证据确定性的主要原因是研究局限性(研究被判定为存在不确定或高偏倚风险)、不一致性(对疼痛强度/严重程度)、不精确性(效应估计值周围的样本量小且置信区间宽)和间接性(人群、干预措施和比较剂的方法学和临床异质性)。
SMT 治疗偏头痛的疗效仍未得到证实。未来,更大、更严格和独立进行的研究可能会降低现有的不确定性。