Liu Yang, Diamond Charlie, Abbott Sam, Wong Kerry, Schmidt Tanja, Edmunds W John, Pebody Richard, Jit Mark
Department of Infectious Disease Epidemiology, Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK.
Centre for Mathematical Modelling of Infectious Diseases, London School of Hygiene and Tropical Medicine, London, UK.
Influenza Other Respir Viruses. 2024 Dec;18(12):e70036. doi: 10.1111/irv.70036.
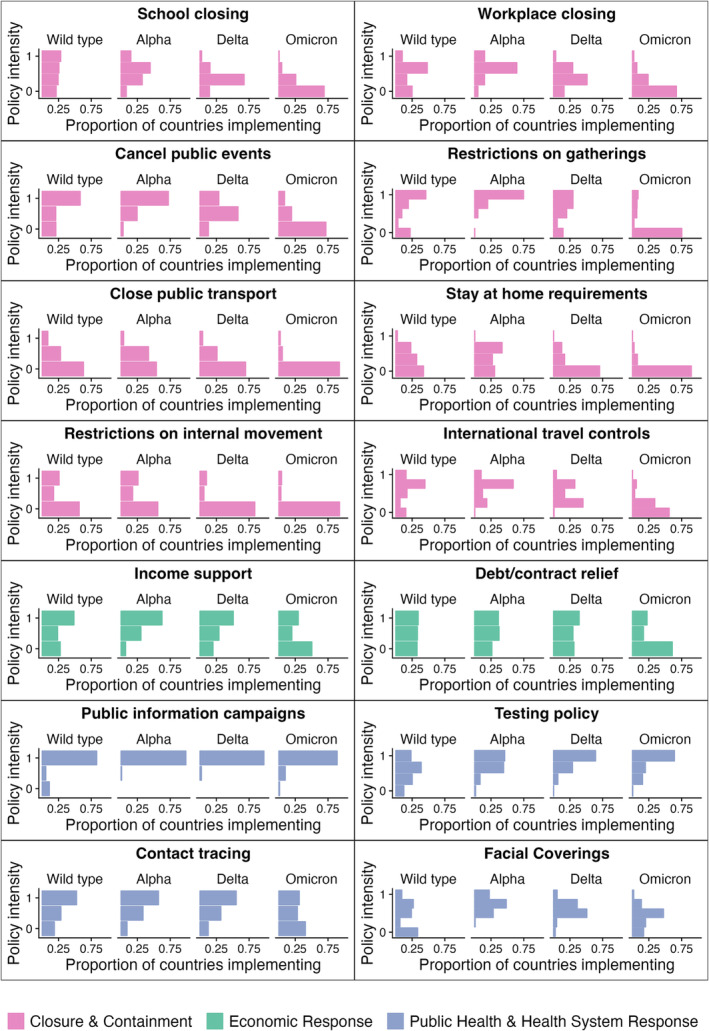
Between 2020 and 2022, countries used a range of different public health and social measures (PHSMs) to reduce the transmission of SARS-CoV-2. The impact of these PHSMs varied as the pandemic progressed, variants of concern (VOCs) emerged, vaccines rolled out and acceptance/uptake rates evolved. In this study, we assessed the impact of PHSMs in the World Health Organization (WHO) European Region during VOC phases.
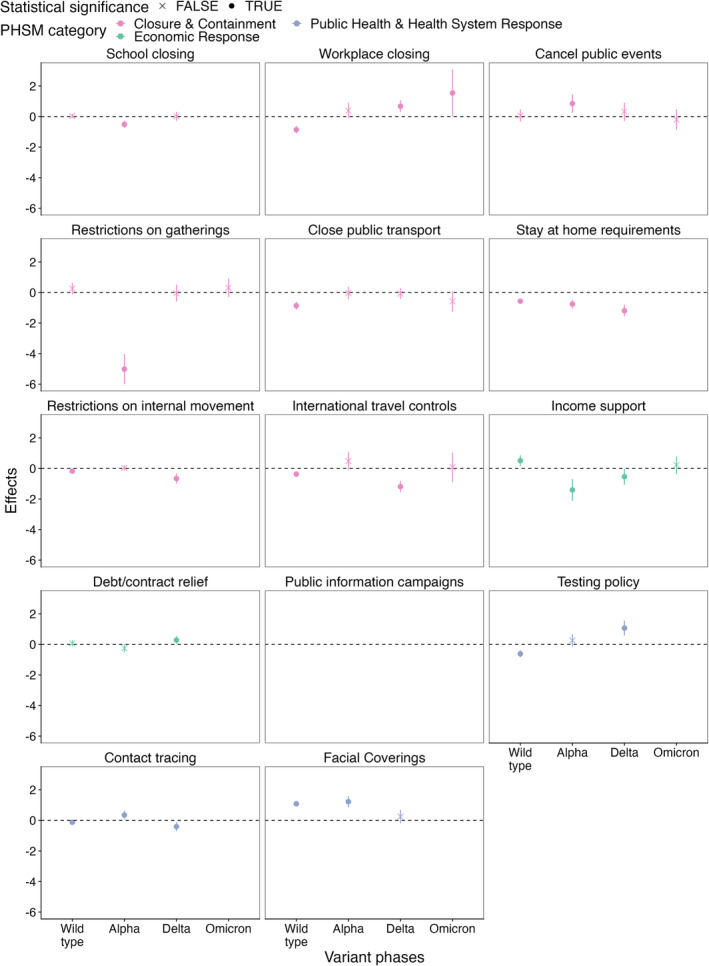
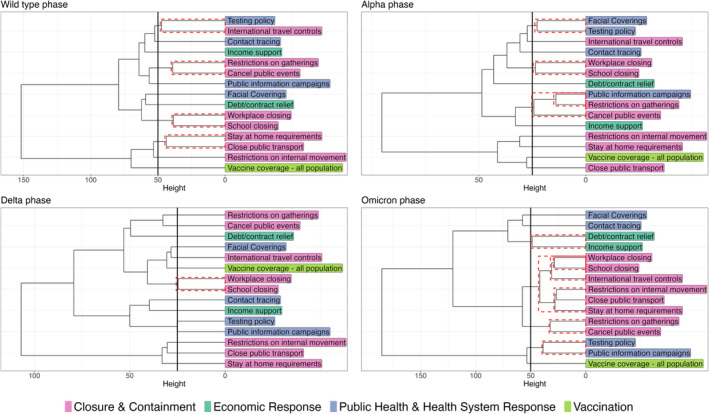
We relied on time series data on genome sequencing, PHSMs, health outcomes and physical contacts. Panel regression models were used to assess the association between PHSMs and SARS-CoV-2 transmission (approximated using time-varying reproduction numbers). The interpretation of these regression models was assisted by hierarchical clustering, which was used to detect the temporal co-occurrence of PHSMs. Generalised linear models were used to check if PHSMs are associated with physical contacts.
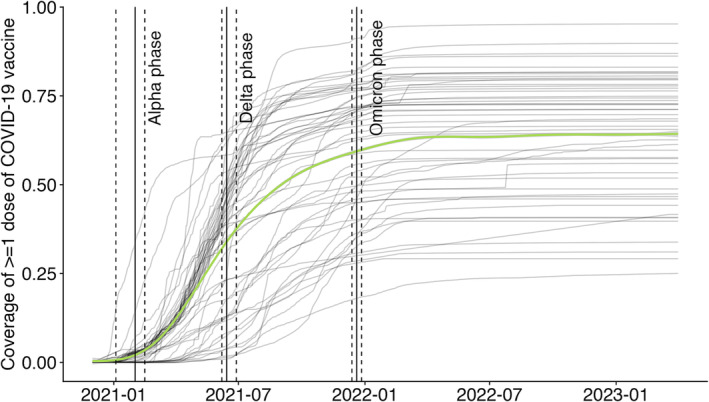
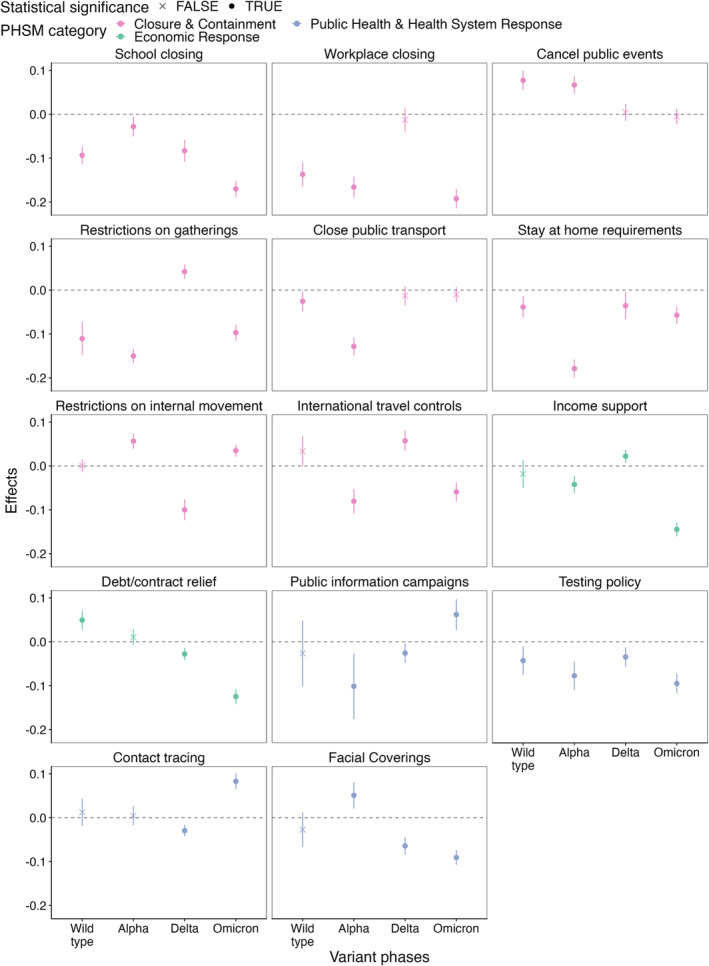
We identified four phases based on the dominating VOC in the WHO European Region: wild type (before early 2021), Alpha (early to mid-2021), Delta (mid-to-late 2021) and Omicron (after late 2021). 'School closure', 'stay-at-home requirement' and 'testing policy' were consistently associated with lower transmission across VOC phases. The impact of most PHSMs varied by VOC phases without clear increasing or decreasing trends as the pandemic progressed. Several PHSMs associated with lower transmission were not associated with fewer physical contacts.
The impact of PHSMs evolved as the pandemic progressed-although without clear trends. The specific mechanisms by which some PHSMs reduce SARS-CoV-2 transmission require further research.
2020年至2022年期间,各国采取了一系列不同的公共卫生和社会措施(PHSMs)来减少严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的传播。随着疫情的发展、关注变异株(VOCs)的出现、疫苗的推出以及接受/接种率的变化,这些公共卫生和社会措施的影响也有所不同。在本研究中,我们评估了公共卫生和社会措施在VOC阶段对世界卫生组织(WHO)欧洲区域的影响。
我们依赖于基因组测序、公共卫生和社会措施、健康结果及身体接触的时间序列数据。使用面板回归模型评估公共卫生和社会措施与SARS-CoV-2传播之间的关联(使用随时间变化的再生数进行近似)。层次聚类有助于对这些回归模型进行解释,用于检测公共卫生和社会措施的时间共现情况。使用广义线性模型检查公共卫生和社会措施是否与身体接触有关。
我们根据WHO欧洲区域中占主导地位的VOC确定了四个阶段:野生型(2021年初之前)、阿尔法(2021年上半年)、德尔塔(2021年下半年)和奥密克戎(2021年末之后)。“学校关闭”“居家要求”和“检测政策”在各VOC阶段均始终与较低的传播率相关。随着疫情发展,大多数公共卫生和社会措施的影响因VOC阶段而异,没有明显的上升或下降趋势。一些与较低传播率相关的公共卫生和社会措施与身体接触减少无关。
随着疫情的发展,公共卫生和社会措施的影响不断演变——尽管没有明显趋势。一些公共卫生和社会措施降低SARS-CoV-2传播率的确切机制需要进一步研究。