Peak Corey M, Lyons Hil, Voorman Arend, Gray Elizabeth J, Cooper Laura V, Blake Isobel M, Hawes Kaija M, Bandyopadhyay Ananda S
Bill & Melinda Gates Foundation, Seattle, WA 98109, USA.
MRC Centre for Global Infectious Disease Analysis, School of Public Health, Imperial College London, London W12 0BZ, UK.
Vaccines (Basel). 2024 Nov 22;12(12):1308. doi: 10.3390/vaccines12121308.
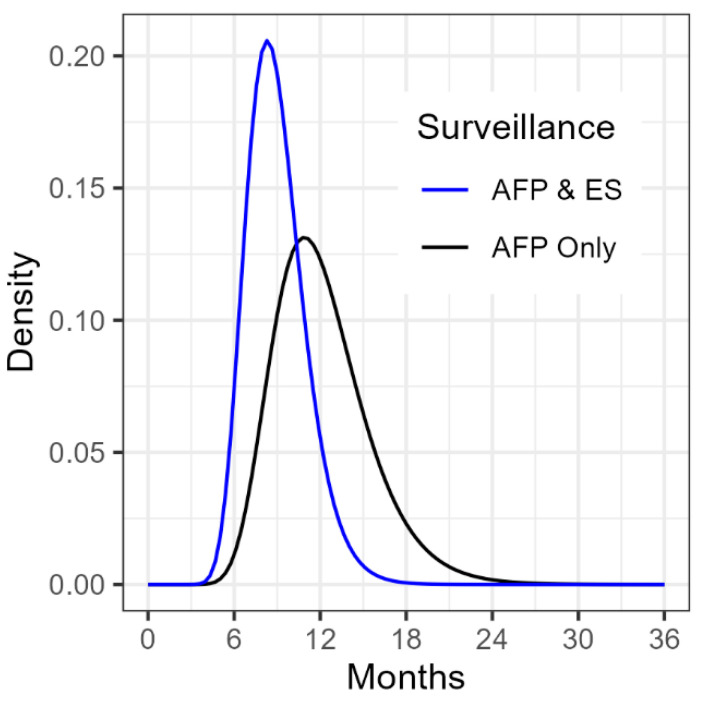
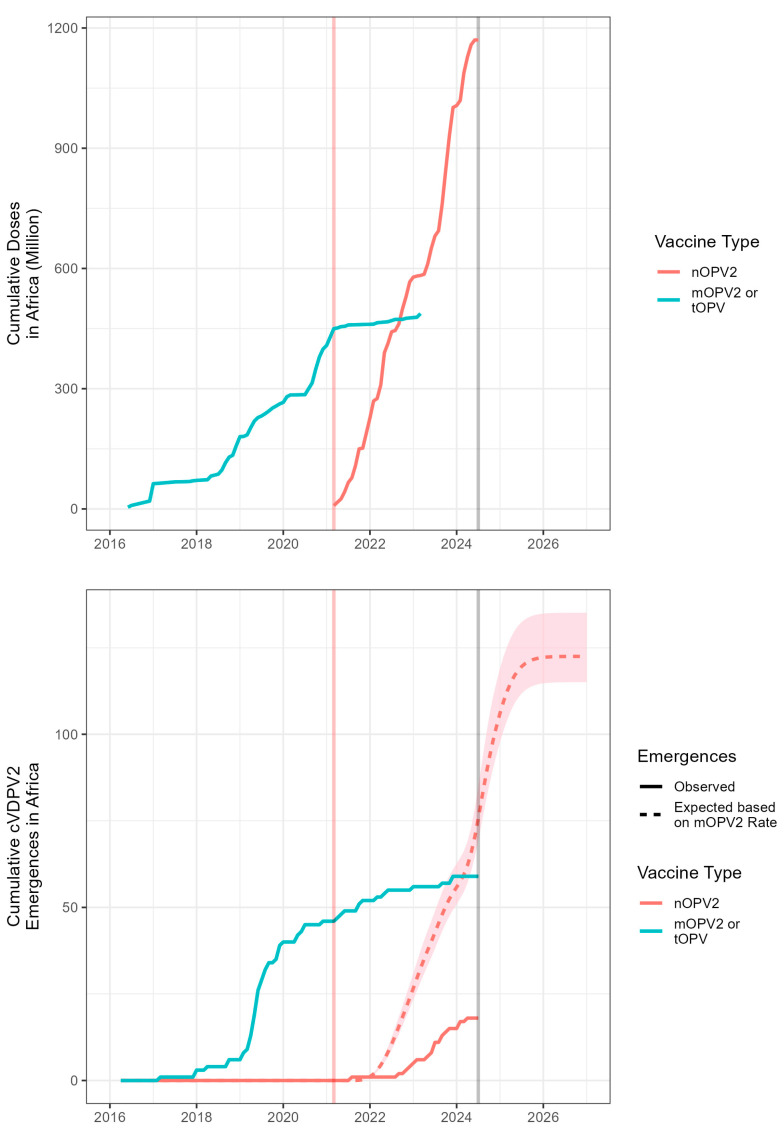
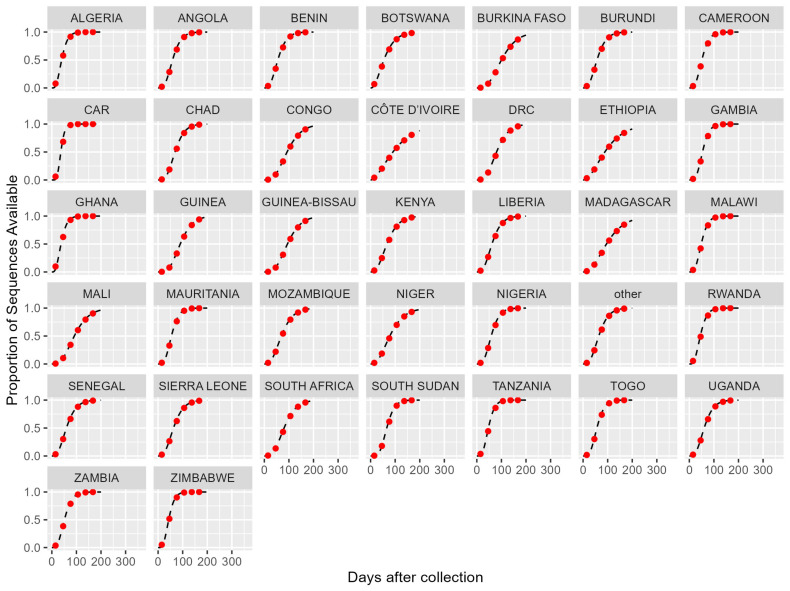
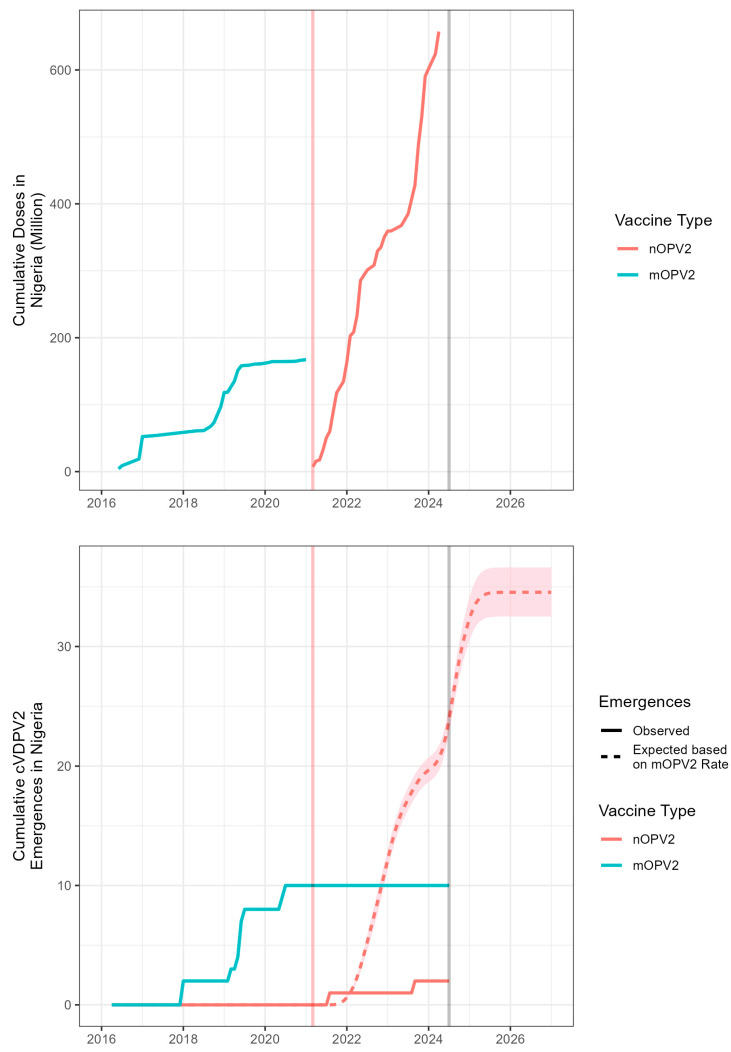
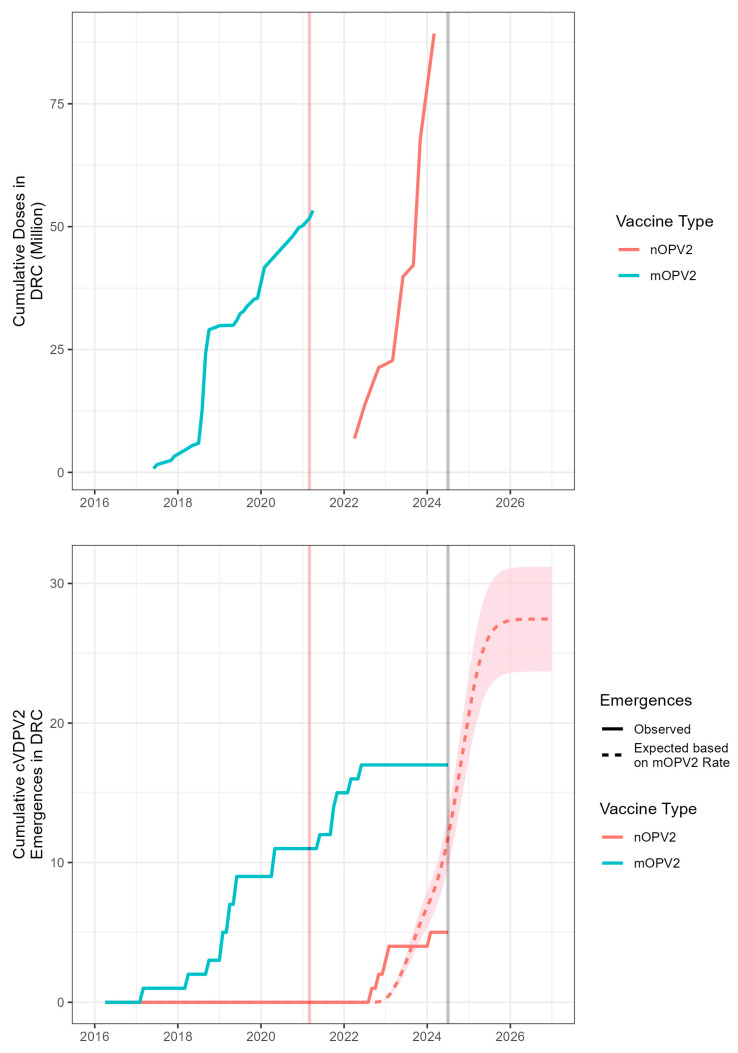
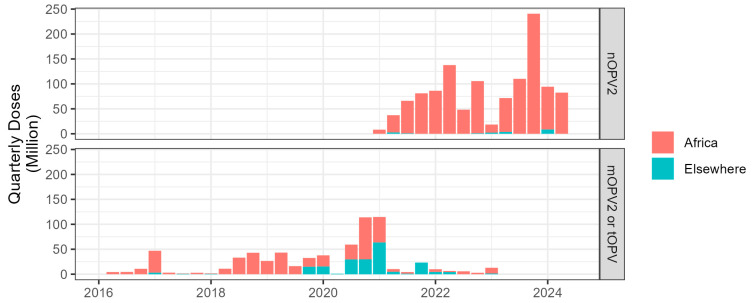
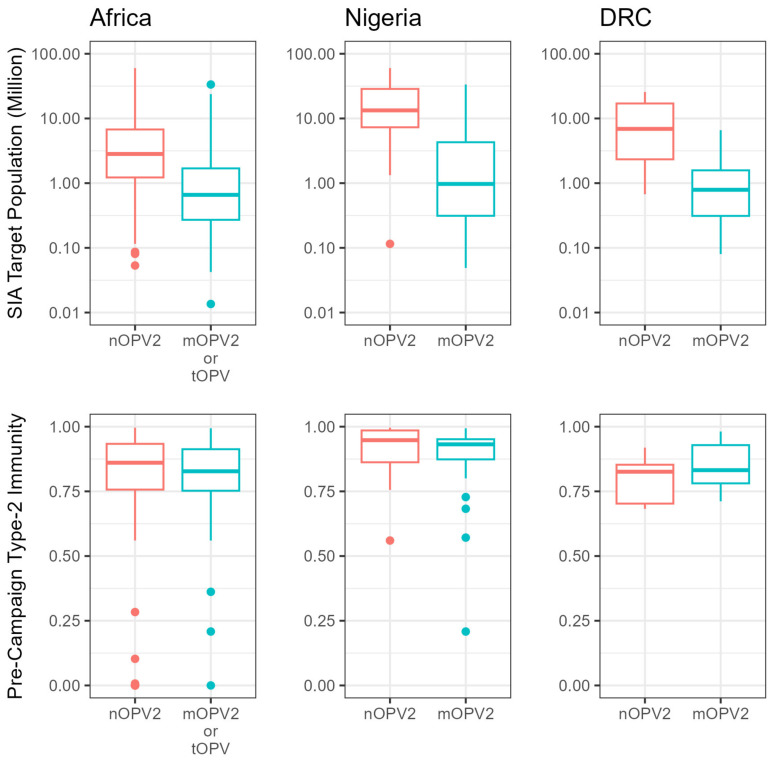
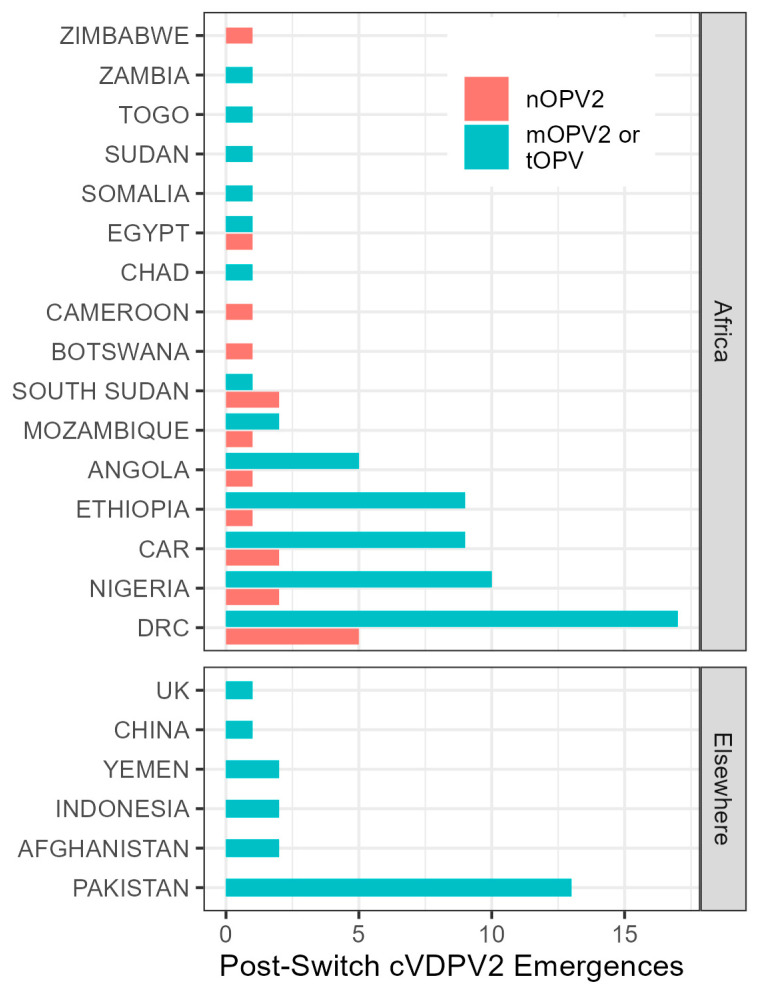
Although wild poliovirus type 2 has been eradicated, the prolonged transmission of the live- attenuated virus contained in the type-2 oral polio vaccine (OPV2) in under-immunized populations has led to the emergence of circulating vaccine-derived poliovirus type 2 (cVDPV2). The novel OPV2 (nOPV2) was designed to be more genetically stable and reduce the chance of cVDPV2 emergence while retaining comparable immunogenicity to the Sabin monovalent OPV2 (mOPV2). This study aimed to estimate the relative reduction in the emergence risk due to the use of nOPV2 instead of mOPV2. Data on OPV2 vaccination campaigns from May 2016 to 1 August 2024 were analyzed to estimate type-2 OPV-induced immunity in children under 5 years of age. Poliovirus surveillance data were used to estimate seeding dates and classify cVDPV2 emergences as mOPV2- or nOPV2-derived. The expected number of emergences if mOPV2 was used instead of nOPV2 was estimated, accounting for the timing and volume of nOPV2 doses, the known risk factors for emergence from mOPV2, and censoring due to the incomplete observation period for more recent nOPV2 doses. As of 1 August 2024, over 98% of the approximately 1.19 billion nOPV2 doses administered globally were in Africa. We estimate that approximately 76 (95% confidence interval 69-85) index isolates of cVDPV2 emergences would be expected to be detected by 1 August 2024 if mOPV2 had been used instead of nOPV2 in Africa. The 18 observed nOPV2-derived emergences represent a 76% (74-79%) lower risk of emergence by nOPV2 than mOPV2 in Africa. The crude global analysis produced similar results. Key limitations include the incomplete understanding of the drivers of heterogeneity in emergence risk across geographies and variance in the per-dose risk of emergence may be incompletely captured using known risk factors. These results are consistent with the accumulating clinical and field evidence showing the enhanced genetic stability of nOPV2 relative to mOPV2, and this approach has been implemented in near-real time to contextualize new findings during the roll-out of this new vaccine. While nOPV2 has resulted in new emergences of cVDPV2, the number of cVDPV2 emergences is estimated to be approximately four-fold lower than if mOPV2 had been used instead.
虽然野生脊髓灰质炎病毒2型已被根除,但在免疫接种不足的人群中,2型口服脊髓灰质炎疫苗(OPV2)中所含减毒活病毒的长期传播导致了2型循环疫苗衍生脊髓灰质炎病毒(cVDPV2)的出现。新型OPV2(nOPV2)的设计目的是在保持与萨宾单价OPV2(mOPV2)相当免疫原性的同时,在基因上更稳定,并降低cVDPV2出现的可能性。本研究旨在估计使用nOPV2而非mOPV2导致的出现风险的相对降低。分析了2016年5月至2024年8月1日期间OPV2疫苗接种运动的数据,以估计5岁以下儿童中2型OPV诱导的免疫力。脊髓灰质炎病毒监测数据用于估计传播日期,并将cVDPV2的出现分类为源自mOPV2或nOPV2。估计了如果使用mOPV2而非nOPV2时的预期出现次数,考虑了nOPV2剂量的时间和数量、mOPV2出现的已知风险因素,以及由于最近nOPV2剂量观察期不完整而进行的截尾。截至2024年8月1日,全球接种的约11.9亿剂nOPV2中,超过98%在非洲。我们估计,如果在非洲使用mOPV而不是nOPV2,到2024年8月1日预计将检测到约76例(95%置信区间69 - 85)cVDPV2出现的指示性分离株。在非洲,观察到的18例源自nOPV2的出现表明,nOPV2出现的风险比mOPV2低76%(74 - 79%)。粗略的全球分析得出了类似的结果。主要局限性包括对不同地区出现风险异质性驱动因素的理解不完整,以及使用已知风险因素可能无法完全捕捉每剂出现风险的差异。这些结果与越来越多的临床和现场证据一致,表明nOPV2相对于mOPV2具有更高的基因稳定性,并且在这种新疫苗推出期间,这种方法已近乎实时地用于将新发现背景化。虽然nOPV2导致了cVDPV2的新出现,但估计cVDPV2出现的数量比使用mOPV2时低约四倍。