Zhou Yanyou, Tao Linfeng, Yang Shengsheng, Li Juntu, Liu Jun
Department of Emergency and Critical Care Medicine, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Gusu School of Nanjing Medical University, Suzhou Clinical Medical Center of Critical Care Medicine, Suzhou, China.
Front Med (Lausanne). 2024 Dec 11;11:1465397. doi: 10.3389/fmed.2024.1465397. eCollection 2024.
Critical illness-associated immune dysfunction (CIID) is prevalent in the ICU and frequently resulted in uncontrollably immune responses. Critical immunological dysfunction is understood to be important, although there are currently no clinically accepted diagnostic criteria for it. Given this, we examined the literature and developed an initial diagnostic criterion that we validated using the MIMIC-IV database.
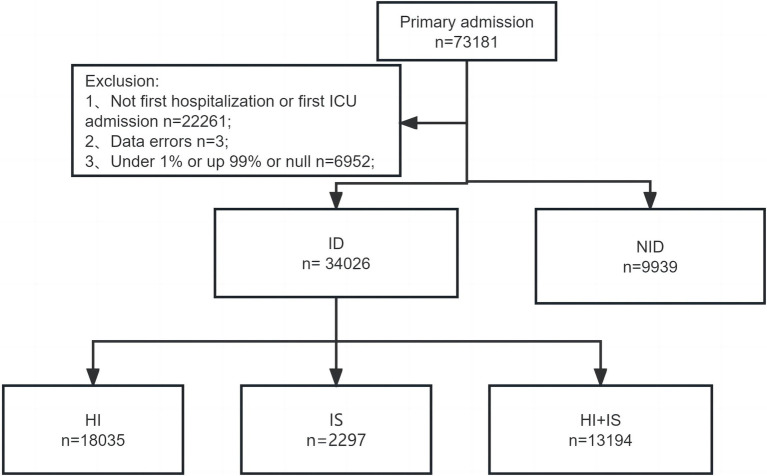
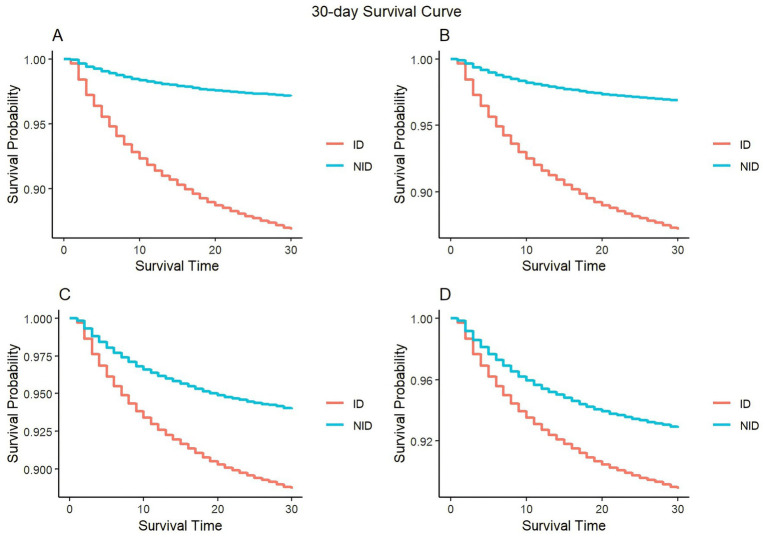
We searched the related literature in the last 32 years. Patients admitted to the ICU for the first time were selected by screening the MIMIC-IV database. Different criteria were used to categorize patients into groups related to immune dysfunction (ID) and non-immune dysfunction (NID). Within the ID group, patients were subdivided into three subgroups: hyperinflammatory (HI), immunosuppression (IS), and a subgroup combining immunosuppression and hyperinflammation (HI+IS). The APACHE II was used to measure the patients' severity. The association between immune dysfunction and mortality after 30 or 180 days was evaluated through the KM curves and COX regression analysis.
By summarizing relevant literature, we proposed the initial diagnostic criteria. The analysis included 43,965 patients, with approximately 77% meeting the diagnostic criteria for CIID. We observed that patients with immune dysfunction possessed higher APACHE II scores and there were differences in peak APACHE II among the three subgroups. When comparing patients' 30-day mortality in the COX model, it is evident that patients in the IS subgroup had the lowest risk and patients in the HI subgroup the greatest risk after accounting for all covariates. In contrast, patients in the IS subgroup had the highest risk of death, those in the HI subgroup had the lowest risk when comparing long-term mortality. In summary, we propose and validate diagnostic criteria related to CIID. Subgroup analyses were carried out, which also revealed variations between the three groups.
The diagnostic criteria were confirmed by the MIMIC-IV database, demonstrating the diagnostic criteria were scientifically valid and reliable.
危重症相关免疫功能障碍(CIID)在重症监护病房(ICU)中普遍存在,并经常导致无法控制的免疫反应。尽管目前尚无临床上公认的诊断标准,但严重免疫功能障碍被认为很重要。鉴于此,我们查阅了文献并制定了初步诊断标准,并使用MIMIC-IV数据库对其进行了验证。
我们检索了过去32年的相关文献。通过筛选MIMIC-IV数据库,选择首次入住ICU的患者。使用不同标准将患者分为免疫功能障碍(ID)组和非免疫功能障碍(NID)组。在ID组中,患者又被细分为三个亚组:高炎症反应(HI)、免疫抑制(IS)以及免疫抑制与高炎症反应合并亚组(HI+IS)。使用急性生理与慢性健康状况评分系统II(APACHE II)来衡量患者的病情严重程度。通过Kaplan-Meier(KM)曲线和COX回归分析评估免疫功能障碍与30天或180天后死亡率之间的关联。
通过总结相关文献,我们提出了初步诊断标准。分析纳入了43965例患者,其中约77%符合CIID诊断标准。我们观察到免疫功能障碍患者的APACHE II评分较高,且三个亚组之间的APACHE II峰值存在差异。在COX模型中比较患者的30天死亡率时,很明显在考虑所有协变量后,IS亚组患者的风险最低,HI亚组患者的风险最高。相比之下,在比较长期死亡率时,IS亚组患者的死亡风险最高,HI亚组患者的风险最低。总之,我们提出并验证了与CIID相关的诊断标准。进行了亚组分析,结果也显示了三组之间的差异。
MIMIC-IV数据库证实了该诊断标准,表明该诊断标准科学有效且可靠。