Boyle Alex B, Shay Denys, Martyn Tanushk, Savage Earle, MacLean Simon B M, Every-Palmer Susanna
Specialty Trainees of New Zealand, Christchurch, New Zealand
Department of Health Policy and Management, Harvard T.H. Chan School of Public Health, Boston, Massachusetts, USA.
BMJ Open. 2025 Jan 15;15(1):e089034. doi: 10.1136/bmjopen-2024-089034.
Burnout syndrome, characterised by emotional exhaustion, depersonalisation and decreased personal accomplishment, is well documented in the medical workforce. This study aimed to investigate the prevalence of burnout in New Zealand resident doctors (doctors who have yet to complete their specialty training).
Cross-sectional survey study of resident doctors in New Zealand.
Distributed by email.
509 resident doctors currently working in New Zealand. Doctors not currently working or those who have completed their specialty training (consultants) were excluded.
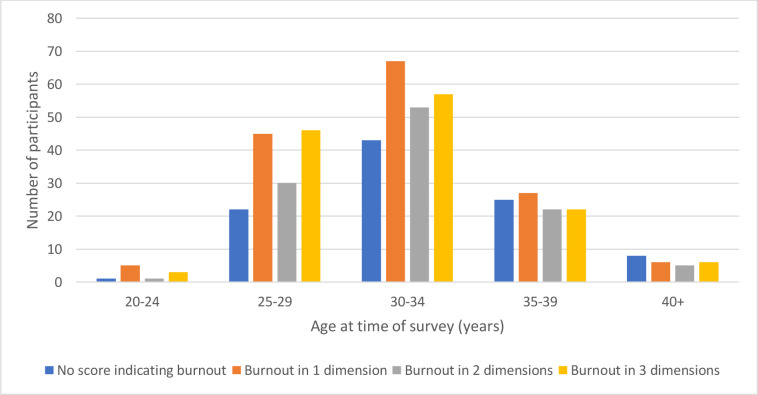
Participants were asked about a number of demographic and work-related factors and to complete the Maslach Burnout Inventory, which measures the three dimensions of burnout: 'Emotional Exhaustion', 'Depersonalisation' and low 'Personal Accomplishment'.
409/509 (80%) of respondents had scores indicating high burnout on at least one dimension. 163 (32%) had high burnout on one dimension, 111 (22%) on two dimensions and 135 (26%) on all three dimensions. Feeling well supported protected against burnout in all three dimensions: emotional exhaustion (OR 0.34, CI 0.19 to 0.60), depersonalisation (OR 0.52, CI 0.31 to 0.86) and decreased personal accomplishment (OR 0.51, CI 0.29 to 0.78). Having a manageable workload protected against emotional exhaustion (OR 0.23, CI 0.13 to 0.37) and depersonalisation (OR 0.39, CI 0.24 to 0.61). Increasing weekly exercise was protective for personal accomplishment (OR 0.846, CI 0.73 to 0.98). Having children was protective for depersonalisation (OR 0.7, CI 0.53 to 0.90). A personal history of depression or anxiety was associated with burnout on all three dimensions: emotional exhaustion (OR 2.86, CI 1.67 to 5.00), depersonalisation (OR 1.66, CI 1.01 to 2.73) and decreased personal accomplishment (OR 1.71, CI 1.05 to 2.80). Alcohol misuse was associated with an increased risk of depersonalisation (OR 1.68, CI 1.08 to 2.62), and feeling inadequately remunerated was associated with emotional exhaustion (OR 2.27, CI 1.28 to 4.17). Qualitative data revealed concerns about poor staffing, inadequate remuneration, a focus on service provision over education, slow career progression and difficulty balancing work and specialty examinations.
Burnout has a high prevalence in New Zealand's resident doctor workforce. Several associations and qualitative themes were identified. These findings may aid in the development of interventions to mitigate burnout in the medical workforce.
职业倦怠综合征以情感耗竭、去人格化和个人成就感降低为特征,在医疗工作者中已有充分记录。本研究旨在调查新西兰住院医生(尚未完成专科培训的医生)中职业倦怠的患病率。
对新西兰住院医生的横断面调查研究。
通过电子邮件分发。
509名目前在新西兰工作的住院医生。未在工作的医生或已完成专科培训的医生(顾问医生)被排除在外。
询问参与者一些人口统计学和工作相关因素,并要求他们完成马氏职业倦怠量表,该量表测量职业倦怠的三个维度:“情感耗竭”、“去人格化”和低“个人成就感”。
409/509(80%)的受访者在至少一个维度上得分表明存在高度职业倦怠。163人(32%)在一个维度上存在高度职业倦怠,111人(22%)在两个维度上存在高度职业倦怠,135人(26%)在所有三个维度上存在高度职业倦怠。感觉得到充分支持可预防所有三个维度的职业倦怠:情感耗竭(比值比0.34,可信区间0.19至0.60)、去人格化(比值比0.52,可信区间0.31至0.86)和个人成就感降低(比值比0.51,可信区间0.29至0.78)。工作量可控可预防情感耗竭(比值比0.23,可信区间0.13至0.37)和去人格化(比值比0.39,可信区间0.24至0.61)。每周增加运动量对个人成就感有保护作用(比值比0.846,可信区间0.73至0.98)。有孩子对去人格化有保护作用(比值比0.7,可信区间0.53至0.90)。有抑郁或焦虑个人史与所有三个维度的职业倦怠相关:情感耗竭(比值比2.86,可信区间1.67至5.00)、去人格化(比值比1.66,可信区间1.01至2.73)和个人成就感降低(比值比1.71,可信区间1.05至2.80)。酗酒与去人格化风险增加相关(比值比1.68,可信区间1.08至2.62),感觉薪酬不足与情感耗竭相关(比值比2.27,可信区间1.28至4.17)。定性数据揭示了对人员配备不足、薪酬不足、注重服务提供而非教育、职业发展缓慢以及难以平衡工作和专科考试的担忧。
职业倦怠在新西兰住院医生群体中患病率很高。确定了几个关联因素和定性主题。这些发现可能有助于制定干预措施以减轻医疗工作者的职业倦怠。