Shah Dimpy P, Thaweethai Tanayott, Karlson Elizabeth W, Bonilla Hector, Horne Benjamin D, Mullington Janet M, Wisnivesky Juan P, Hornig Mady, Shinnick Daniel J, Klein Jonathan D, Erdmann Nathaniel B, Brosnahan Shari B, Lee-Iannotti Joyce K, Metz Torri D, Maughan Christine, Ofotokun Ighovwerha, Reeder Harrison T, Stiles Lauren E, Shaukat Aasma, Hess Rachel, Ashktorab Hassan, Bartram Logan, Bassett Ingrid V, Becker Jacqueline H, Brim Hassan, Charney Alexander W, Chopra Tananshi, Clifton Rebecca G, Deeks Steven G, Erlandson Kristine M, Fierer Daniel S, Flaherman Valerie J, Fonseca Vivian, Gander Jennifer C, Hodder Sally L, Jacoby Vanessa L, Kotini-Shah Pavitra, Krishnan Jerry A, Kumar Andre, Levy Bruce D, Lieberman David, Lin Jenny J, Martin Jeffrey N, McComsey Grace A, Moukabary Talal, Okumura Megumi J, Peluso Michael J, Rosen Clifford J, Saade George, Shah Pankil K, Sherif Zaki A, Taylor Barbara S, Tuttle Katherine R, Urdaneta Alfredo E, Wallick Julie A, Wiley Zanthia, Zhang David, Horwitz Leora I, Foulkes Andrea S, Singer Nora G
Long School of Medicine, University of Texas Health Science Center, San Antonio.
Massachusetts General Hospital Biostatistics, Somerville.
JAMA Netw Open. 2025 Jan 2;8(1):e2455430. doi: 10.1001/jamanetworkopen.2024.55430.
A substantial number of individuals worldwide experience long COVID, or post-COVID condition. Other postviral and autoimmune conditions have a female predominance, but whether the same is true for long COVID, especially within different subgroups, is uncertain.
To evaluate sex differences in the risk of developing long COVID among adults with SARS-CoV-2 infection.
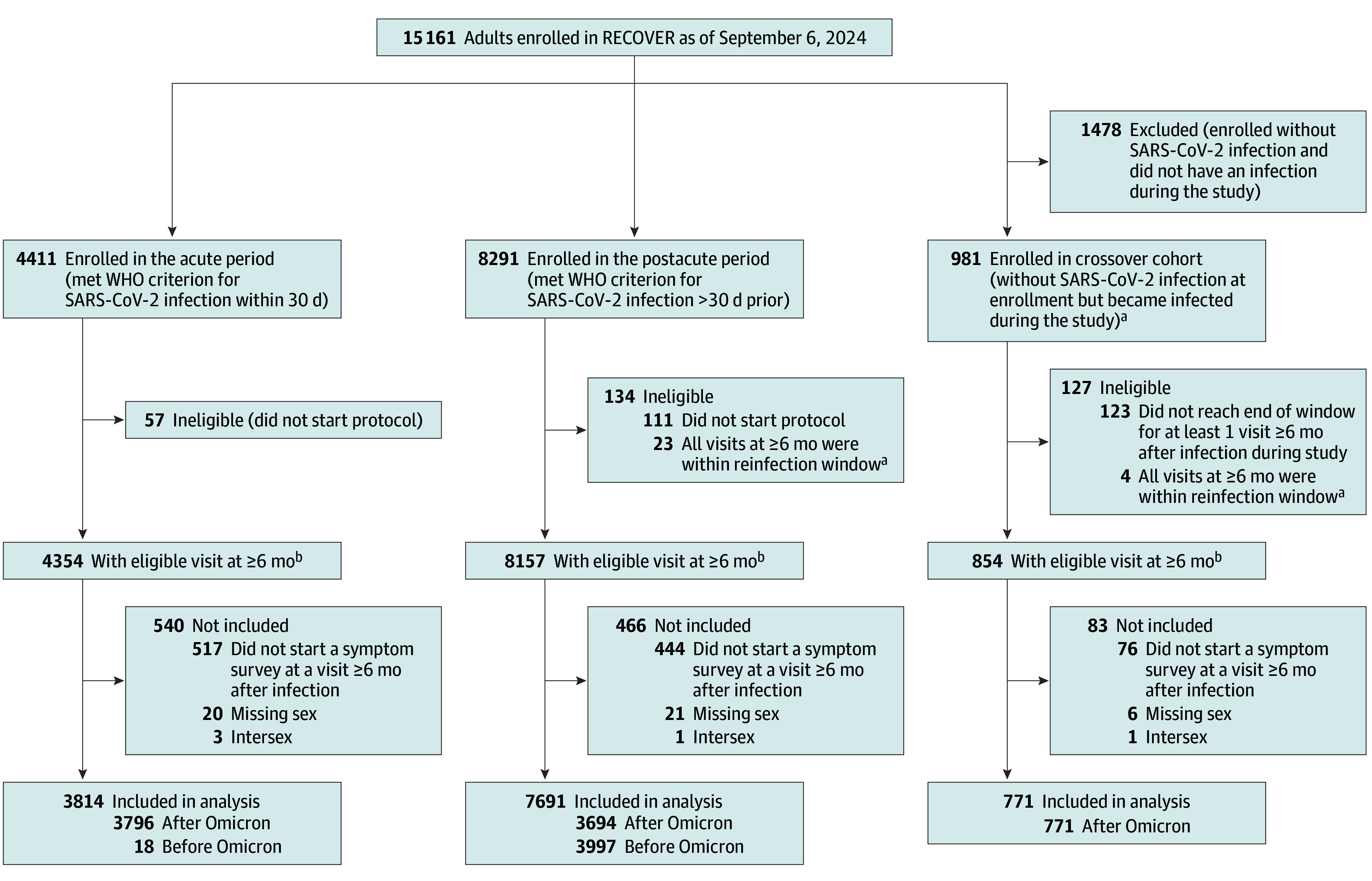
DESIGN, SETTING, AND PARTICIPANTS: This cohort study used data from the National Institutes of Health (NIH) Researching COVID to Enhance Recovery (RECOVER)-Adult cohort, which consists of individuals enrolled in and prospectively followed up at 83 sites in 33 US states plus Washington, DC, and Puerto Rico. Data were examined from all participants enrolled between October 29, 2021, and July 5, 2024, who had a qualifying study visit 6 months or more after their initial SARS-CoV-2 infection.
Self-reported sex (male, female) assigned at birth.
Development of long COVID, measured using a self-reported symptom-based questionnaire and scoring guideline at the first study visit that occurred at least 6 months after infection. Propensity score matching was used to estimate risk ratios (RRs) and risk differences (95% CIs). The full model included demographic and clinical characteristics and social determinants of health, and the reduced model included only age, race, and ethnicity.
Among 12 276 participants who had experienced SARS-CoV-2 infection (8969 [73%] female; mean [SD] age at infection, 46 [15] years), female sex was associated with higher risk of long COVID in the primary full (RR, 1.31; 95% CI, 1.06-1.62) and reduced (RR, 1.44; 95% CI, 1.17-1.77) models. This finding was observed across all age groups except 18 to 39 years (RR, 1.04; 95% CI, 0.72-1.49). Female sex was associated with significantly higher overall long COVID risk when the analysis was restricted to nonpregnant participants (RR, 1.50; 95%: CI, 1.27-1.77). Among participants aged 40 to 54 years, the risk ratio was 1.42 (95% CI, 0.99-2.03) in menopausal female participants and 1.45 (95% CI, 1.15-1.83) in nonmenopausal female participants compared with male participants.
In this prospective cohort study of the NIH RECOVER-Adult cohort, female sex was associated with an increased risk of long COVID compared with male sex, and this association was age, pregnancy, and menopausal status dependent. These findings highlight the need to identify biological mechanisms contributing to sex specificity to facilitate risk stratification, targeted drug development, and improved management of long COVID.
全球有相当数量的人经历长期新冠,即新冠后状况。其他病毒感染后和自身免疫性疾病女性更为常见,但长期新冠是否如此,尤其是在不同亚组中,尚不确定。
评估感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的成年人发生长期新冠风险的性别差异。
设计、地点和参与者:这项队列研究使用了美国国立卫生研究院(NIH)的“研究新冠以促进康复(RECOVER)-成人队列”的数据,该队列由在美国33个州加上华盛顿特区和波多黎各的83个地点招募并进行前瞻性随访的个体组成。对2021年10月29日至2024年7月5日期间入组的所有参与者的数据进行了检查,这些参与者在首次感染SARS-CoV-2后6个月或更长时间进行了符合条件的研究访视。
出生时自我报告的性别(男性、女性)。
长期新冠的发生情况,在感染后至少6个月进行的首次研究访视时,使用基于自我报告症状的问卷和评分指南进行测量。倾向评分匹配用于估计风险比(RR)和风险差异(95%置信区间)。完整模型包括人口统计学和临床特征以及健康的社会决定因素,简化模型仅包括年龄、种族和民族。
在12276名经历过SARS-CoV-2感染的参与者中(8969名[73%]为女性;感染时的平均[标准差]年龄为46[15]岁),在主要的完整模型(RR,1.31;95%置信区间,1.06 - 1.62)和简化模型(RR,1.44;95%置信区间,1.17 - 1.77)中,女性与长期新冠的较高风险相关。除18至39岁年龄组外(RR,1.04;95%置信区间,0.72 - 1.49),在所有年龄组中均观察到这一发现。当分析仅限于未怀孕参与者时,女性与总体长期新冠风险显著更高相关(RR,1.50;95%:置信区间,1.27 - 1.77)。在40至54岁的参与者中,与男性参与者相比,绝经后女性参与者的风险比为1.42(95%置信区间,0.99 - 2.03),未绝经女性参与者的风险比为1.45(95%置信区间,1.15 - 1.83)。
在这项针对NIH RECOVER - 成人队列的前瞻性队列研究中,与男性相比,女性发生长期新冠的风险增加,且这种关联取决于年龄、妊娠和绝经状态。这些发现凸显了确定导致性别特异性的生物学机制的必要性,以促进风险分层、靶向药物开发以及改善长期新冠的管理。