Kebede Dejene Atinafu, Woyimo Tamirat Godebo, Geleta Megersa Negesa, Chiri Seifu Bacha, Asefa Elsah Tegene, Tukeni Kedir Negesso
Division of Cardiology, Department of Internal Medicine, Haramaya University, Harar, Ethiopia.
Division of Cardiology, Department of Internal Medicine, Jimma University, Jimma, Ethiopia.
Front Cardiovasc Med. 2025 Feb 25;12:1520899. doi: 10.3389/fcvm.2025.1520899. eCollection 2025.
Acute coronary syndrome refers to a group of diseases characterized by sudden, decreased blood supply to the heart muscle that results in cell death, also known as acute myocardial infarction. This results in severe chest pain or discomfort, with the subsequent release of cardiac biomarkers, and alterations in the electrocardiogram. It can cause diminished heart function and mortality if not treated properly with suitable measures. Despite the fact that percutaneous coronary intervention is the standard of care in one subset of acute coronary syndrome, significant number of patients were treated medically due to the limited service in the setting. The purpose of this study was to look at the patterns of acute coronary syndrome (ACS), as well as the management and outcomes of these patients in two Ethiopian tertiary institutions.
A four-year retrospective study was undertaken on 308 patients with acute coronary syndrome, at two tertiary hospitals located in Ethiopia's capital-Addis Ababa.
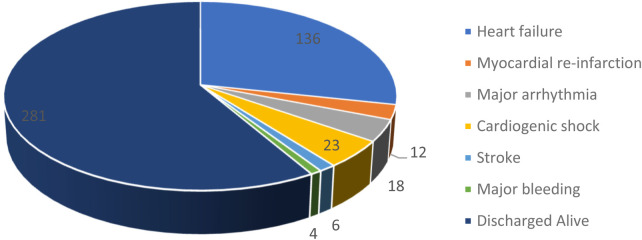
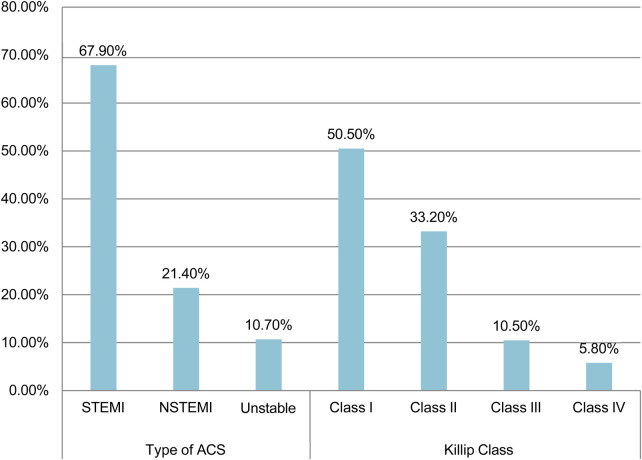
Of the 308 patients 72.4% were male, with the average age of 56.3 ± 13.5 years. Hypertension and diabetes were the two most common risk factors identified. The average time to present to the emergency room after symptom onset was 3.7 (SD ± 3.2) days. The majority of patients (67.9%) have been diagnosed with ST- Elevated Myocardial Infarction and were classified as Killip class I. Percutaneous Coronary Intervention was performed for 12.3% of patients, with the remaining receiving medical care. The average hospital stay was 8.51 (SD ± 7.2) days while In-hospital mortality was 8.8%. Tachycardia of >140 (AOR = 7.50, 95% CI: 1.36, 41.57), any degree of left ventricular dysfunction, Killip class IV (AOR = 6.03, 95% CI: 1.27, 28.61), and non-initiation of betablockers (AOR = 0.17,95% CI: 0.05, 0.63) were significantly associated with increased in-hospital mortality.
急性冠状动脉综合征是指一组以心肌血液供应突然减少导致细胞死亡为特征的疾病,也称为急性心肌梗死。这会导致严重的胸痛或不适,随后会释放心脏生物标志物,并出现心电图改变。如果不采取适当措施进行治疗,可能会导致心脏功能下降和死亡。尽管经皮冠状动脉介入治疗是急性冠状动脉综合征一部分患者的标准治疗方法,但由于该地区服务有限,仍有相当数量的患者接受药物治疗。本研究的目的是观察急性冠状动脉综合征(ACS)的模式,以及这两家埃塞俄比亚三级医疗机构中这些患者的治疗和预后情况。
对位于埃塞俄比亚首都亚的斯亚贝巴的两家三级医院的308例急性冠状动脉综合征患者进行了为期四年的回顾性研究。
308例患者中,72.4%为男性,平均年龄为56.3±13.5岁。高血压和糖尿病是确定的两个最常见危险因素。症状出现后到急诊室就诊的平均时间为3.7(标准差±3.2)天。大多数患者(67.9%)被诊断为ST段抬高型心肌梗死,并被归类为Killip I级。12.3%的患者接受了经皮冠状动脉介入治疗,其余患者接受药物治疗。平均住院时间为8.51(标准差±7.2)天,住院死亡率为8.8%。心率>140(调整后比值比=7.50,95%可信区间:1.36,41.57)、任何程度的左心室功能障碍、Killip IV级(调整后比值比=6.03,95%可信区间:1.27,28.61)以及未开始使用β受体阻滞剂(调整后比值比=0.17,95%可信区间:0.05,0.63)与住院死亡率增加显著相关。