Desai Akshay S, Jhund Pardeep S, Vaduganathan Muthiah, Claggett Brian L, Cunningham Jonathan W, Pabon Maria A, Lam Carolyn S P, Senni Michele, Shah Sanjiv, Voors Adriaan A, Zannad Faiez, Pitt Bertram, Amarante Flaviana, Lay-Flurrie James, Scheerer Markus F, Lage Andrea, McMurray John J V, Solomon Scott D
Cardiovascular Division, Brigham and Women's Hospital, Boston, Massachusetts.
British Heart Foundation Cardiovascular Research Centre, University of Glasgow, Glasgow, United Kingdom.
JAMA Cardiol. 2025 Mar 30. doi: 10.1001/jamacardio.2025.0860.
The mode of death in patients with heart failure with mildly reduced ejection fraction (HFmrEF) or heart failure with preserved ejection fraction (HFpEF) remains poorly understood and may vary by EF.
To evaluate the mode of death according to EF and the treatment effect of finerenone on cause-specific mortality in patients with HFmrEF/HFpEF.
DESIGN, SETTING, AND PARTICIPANTS: This was a prespecified secondary analysis of the Finerenone Trial to Investigate Efficacy and Safety Superior to Placebo in Patients With Heart Failure (FINEARTS-HF) randomized clinical trial, which evaluated clinical outcomes in 6001 patients with HF and EF greater than or equal to 40% randomly assigned to finerenone or placebo. The mode of death in relation to baseline EF categories (<50%, ≥50-<60%, and ≥60%) was examined, and the effect of randomized treatment on cause-specific death in Cox regression models was assessed. Data analysis was conducted between September 2024 and January 2025.
Finerenone vs placebo.
Mode of death as centrally adjudicated by a clinical end points committee.
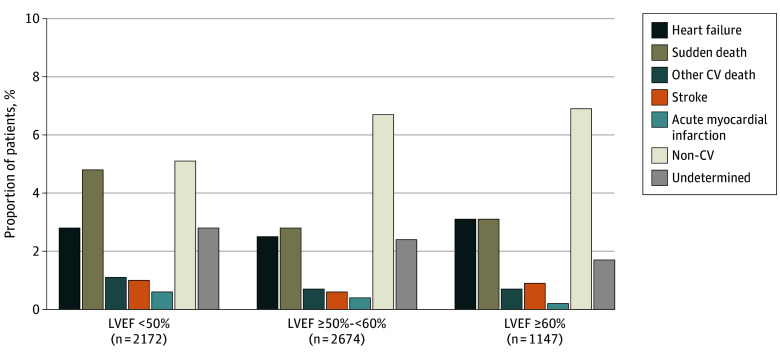
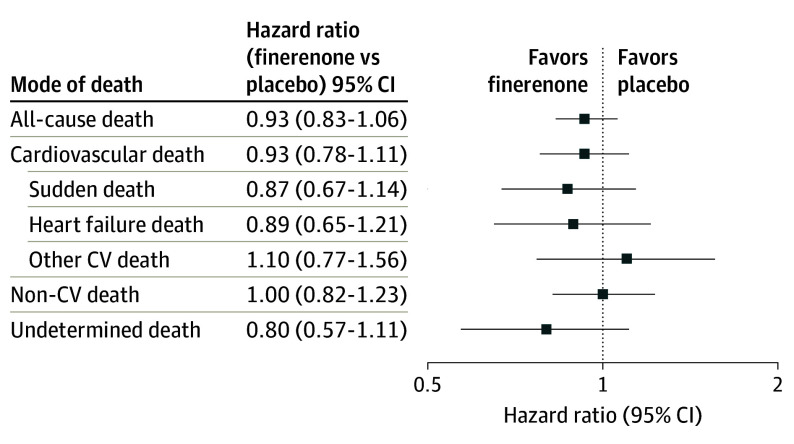
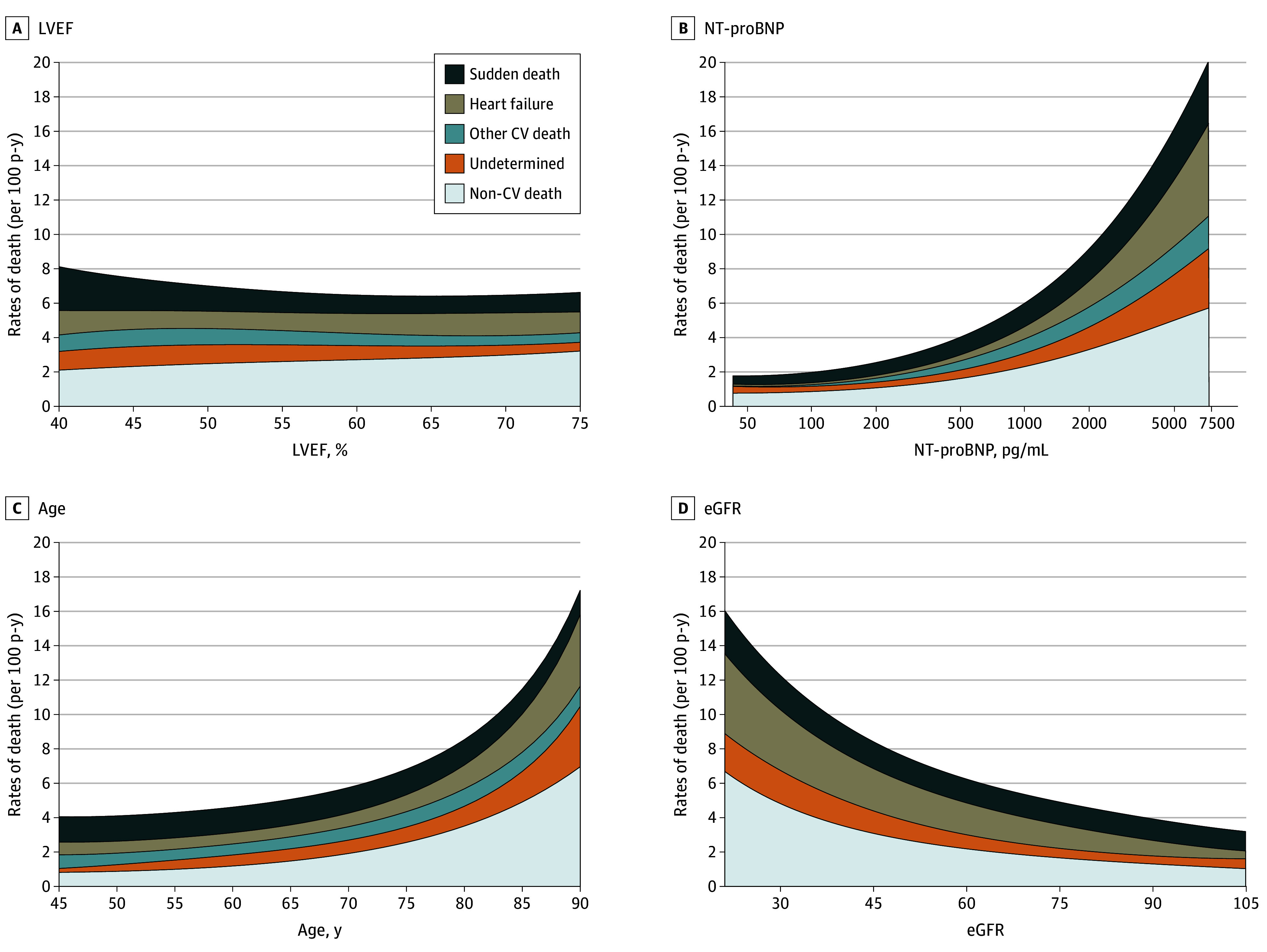
Of 1013 patients (16.9%; median [IQR] age, 76 [69-82] years; 594 male [58.6%]) who died during median (IQR) follow-up of 32 (23-36) months, mode of death was ascribed to cardiovascular causes in 502 (49.6%), noncardiovascular causes in 368 (36.3%), and undetermined cause in 143 (14.1%). Of cardiovascular deaths, 215 (42.8%) were due to sudden death, 163 (32.4%) to HF, 48 (9.6%) to stroke, 25 (5.0%) to myocardial infarction, and 51 (10.2%) to other cardiovascular causes. The proportion of all-cause, cardiovascular, and sudden death was higher in those with EF less than 50%. The proportion of deaths related to HF was similar across EF categories, and the proportion of deaths due to myocardial infarction, stroke, and other cardiovascular causes was low regardless of EF. Randomization to finerenone did not significantly reduce death or cause-specific death compared with placebo in any EF category.
Among patients with HFmrEF/HFpEF in the FINEARTS-HF randomized clinical trial, higher proportions of cardiovascular and overall mortality in those with EF less than 50% were related principally to higher proportions of sudden death. A clear treatment effect of finerenone on cardiovascular or cause-specific mortality was not identified, although the trial was likely underpowered for these outcomes.
ClinicalTrials.gov Identifier: NCT04435626.
射血分数轻度降低的心力衰竭(HFmrEF)或射血分数保留的心力衰竭(HFpEF)患者的死亡方式仍未得到充分了解,且可能因射血分数而异。
根据射血分数评估HFmrEF/HFpEF患者的死亡方式以及非奈利酮对特定病因死亡率的治疗效果。
设计、设置和参与者:这是一项对非奈利酮治疗心力衰竭患者疗效和安全性优于安慰剂的研究(FINEARTS-HF)随机临床试验的预先指定的二次分析,该试验评估了6001例心力衰竭且射血分数大于或等于40%的患者随机分配接受非奈利酮或安慰剂后的临床结局。研究了与基线射血分数类别(<50%、≥50-<60%和≥60%)相关的死亡方式,并在Cox回归模型中评估了随机治疗对特定病因死亡的影响。数据分析于2024年9月至2025年1月进行。
非奈利酮与安慰剂。
由临床终点委员会进行集中判定的死亡方式。
在中位(IQR)随访32(23-36)个月期间死亡的1013例患者(16.9%;中位[IQR]年龄,76[69-82]岁;594例男性[58.6%])中,502例(49.6%)的死亡归因于心血管原因,368例(36.3%)归因于非心血管原因,143例(14.1%)归因于原因不明。在心血管死亡中,215例(42.8%)死于猝死;163例(32.4%)死于心力衰竭;48例(9.6%)死于中风;25例(5.0%)死于心肌梗死;51例(10.2%)死于其他心血管原因。射血分数低于50%的患者全因、心血管和猝死的比例更高。各射血分数类别中与心力衰竭相关的死亡比例相似,无论射血分数如何,因心肌梗死、中风和其他心血管原因导致的死亡比例都较低。与安慰剂相比,在任何射血分数类别中,随机分配接受非奈利酮治疗均未显著降低死亡或特定病因死亡。
在FINEARTS-HF随机临床试验的HFmrEF/HFpEF患者中,射血分数低于50%的患者心血管和总体死亡率较高主要与猝死比例较高有关。未发现非奈利酮对心血管或特定病因死亡率有明确的治疗效果,尽管该试验可能在这些结局方面的检验效能不足。
ClinicalTrials.gov标识符:NCT04435626。