Tian Guo, Zheng Yang, He Yinghua, Chen Can, Zhang Xiaobao, Du Yuxia, Yang Shigui, Jiang Tianan, Li Lanjuan
State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, National Medical Center for Infectious Diseases, Zhejiang University School of Medicine, 79 Qingchun Rd, Hangzhou City, 310003, China.
Department of Clinical Pharmacy, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, China.
BMC Infect Dis. 2025 Apr 8;25(1):483. doi: 10.1186/s12879-025-10881-y.
This study aimed to evaluate the epidemiological trends and spatial-temporal distribution of hepatitis C virus (HCV) in mainland China.
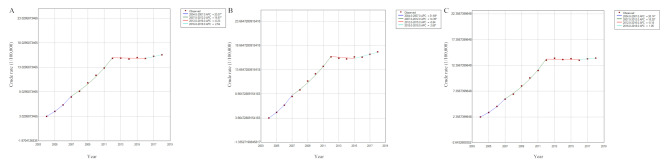
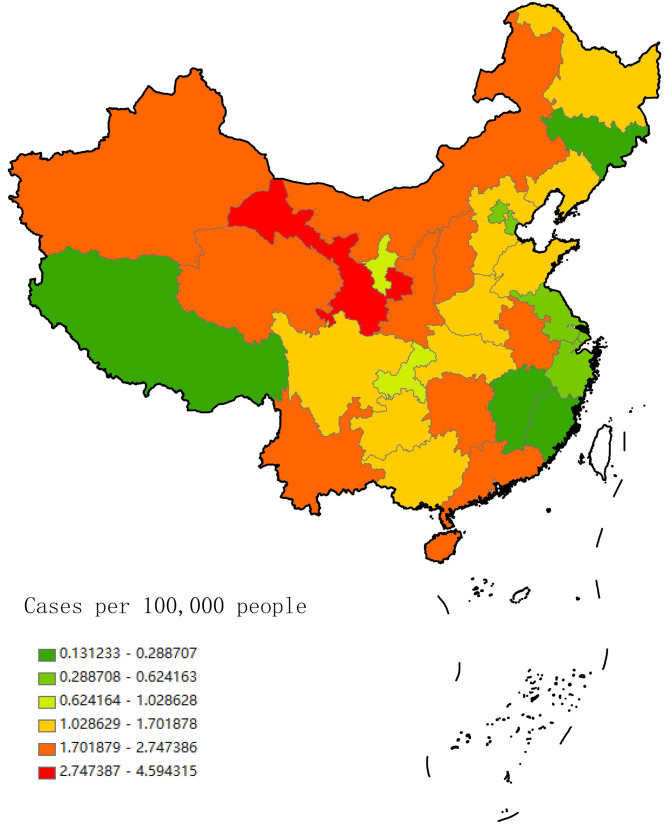
HCV monthly incidence surveillance data from 2004 to 2018 was mainly available from the Public Health Sciences Data Center of China. Five models (Bayesian age-period-cohort, BAPC; Auto-regressive integrated moving average, Auto_arima; Exponential smoothing, ETS; Prophet; Earth) were used to forecast the incidence. Temporal-spatial scanning analysis was conducted to visualize the grading of hepatitis C incidence in mainland China.
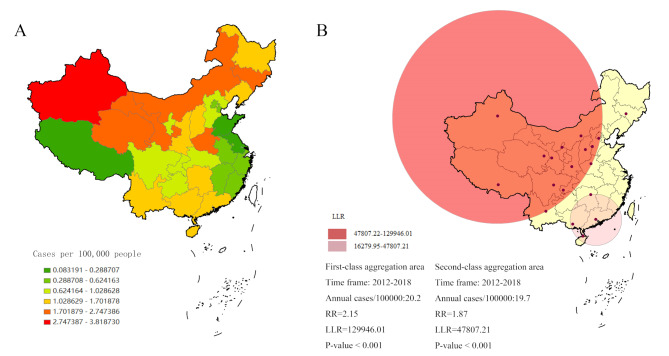
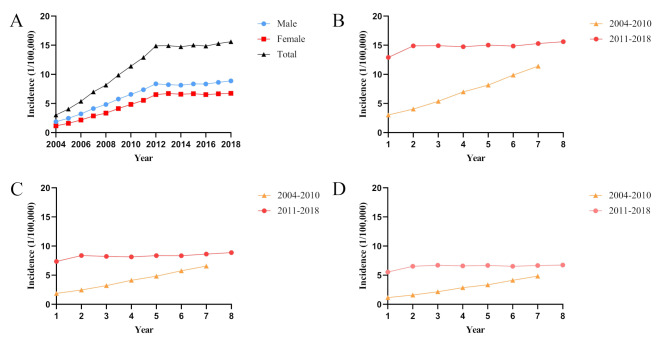
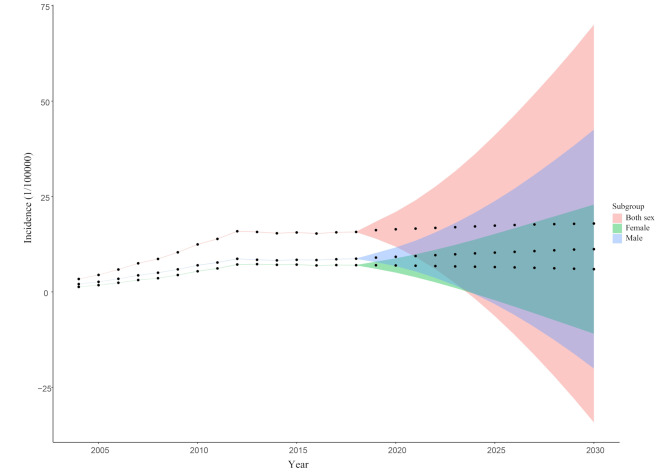
This study observed 180 months of data from January 2004 and December 2018. A total of 2,278,280 hepatitis C cases and 1771 deaths were reported, with an average annual reported incidence rate of 11.24/100,000. The BAPC model indicated that the indexes (mean absolute error, MAE; mean absolute percentage error, MAPE; mean squared error, MSE; root mean square error, RMSE) in the BAPC model were better than those of the other models (4.33 × 10, 0.03, 2.34 × 10, 4.84 × 10), and annual reported HCV incidence in mainland China would remain at a high level of 17.92/100,000 until 2030. Spatial-temporal aggregation analysis indicated that the time range of the first-class aggregation area was from January 1, 2012 to December 31, 2018, and the aggregation area was in Xinjiang, Qinghai, Gansu, Tibet, Ningxia, Inner Mongolia, Sichuan, Shaanxi, Shanxi, Chongqing, Hebei, Beijing, Henan and Yunnan provinces (relative risk, RR = 2.15, log-likelihood ratio, LLR = 129946.01, P < 0.001).
In summary, this study showed that the incidence of HCV in mainland China continued to be high, and BAPC model suggested that this trend will continue until at least 2030. In order to effectively control the HCV epidemic, it was necessary to strengthen blood safety management, expand screening for high-risk population, improve public awareness of HCV, and provide timely and effective antiviral treatment in potentially high-risk areas.
本研究旨在评估中国大陆丙型肝炎病毒(HCV)的流行病学趋势及时空分布。
2004年至2018年的HCV月度发病监测数据主要来自中国公共卫生科学数据中心。使用了五种模型(贝叶斯年龄-时期-队列模型,BAPC;自回归积分滑动平均模型,Auto_arima;指数平滑模型,ETS;Prophet模型;Earth模型)来预测发病率。进行时空扫描分析以直观呈现中国大陆丙型肝炎发病率的分级情况。
本研究观察了2004年1月至2018年12月共180个月的数据。共报告了2,278,280例丙型肝炎病例和1771例死亡,年均报告发病率为11.24/10万。BAPC模型表明,该模型中的指标(平均绝对误差,MAE;平均绝对百分比误差,MAPE;均方误差,MSE;均方根误差,RMSE)优于其他模型(4.33×10,0.03,2.34×10,4.84×10),并且中国大陆HCV的年度报告发病率在2030年前将维持在17.92/10万的高水平。时空聚集分析表明,一级聚集区的时间范围为2012年1月1日至2018年12月31日,聚集区包括新疆、青海、甘肃、西藏、宁夏、内蒙古、四川、陕西、山西、重庆、河北、北京、河南和云南等省份(相对风险,RR = 2.15,对数似然比,LLR = 129946.01,P < 0.001)。
总之,本研究表明中国大陆HCV发病率持续处于高位,BAPC模型显示这一趋势至少将持续到2030年。为有效控制HCV疫情,有必要加强血液安全管理,扩大高危人群筛查,提高公众对HCV的认识,并在潜在高危地区提供及时有效的抗病毒治疗。