Leal-Méndez Francisco, Lewén Anders, Gu Amanda, Hånell Anders, Holmberg Lina, Enblad Per, Linder Fredrik, Wettervik Teodor Svedung
Department of Medical Sciences, Section of Neurosurgery, Uppsala University, 751 85, Uppsala, Sweden.
Department of Surgical Sciences, Section of Vascular Surgery, Uppsala University, 751 85, Uppsala, Sweden.
Acta Neurochir (Wien). 2025 May 8;167(1):134. doi: 10.1007/s00701-025-06557-w.
Sweden covers a large land area, but is sparsely populated. The country is divided into six heterogenous healthcare regions, each with different geographic conditions and referral patterns when it comes to traumatic brain injury (TBI). This study aimed to explore the variation in demography, injury patterns, care pathways, management, and mortality (30 d) for TBI patients within the country.
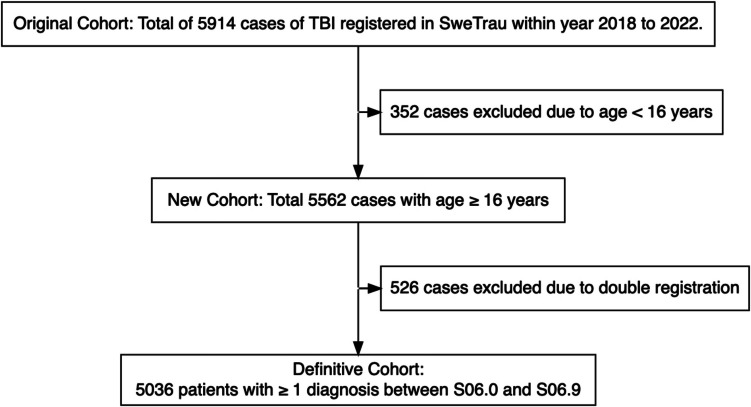
A nationwide, observational study, using data from the Swedish Trauma Registry (SweTrau) between 2018-2022, was performed. A total of 5036 TBI patients were included. Data on demography, admission status (through Glasgow Coma Scale [GCS] value at arrival at first managing hospital), injury-related variables, and mortality (30 d) were evaluated.
The median age was 65 years (interquartile range 46-78), and the majority of patients were male, had sustained fall-related injuries, and were conscious upon admission. Slight, but significant differences (p < 0.05) existed among the regions in these variables. In multivariate logistic regression models, the healthcare region (p < 0.05) was independently associated with patient referral to a university hospital (as compared to care at a local hospital alone), craniotomy rate, and receiving an intracranial pressure-monitoring device, after adjustment for demographic and injury variables. In similar regressions regarding mortality, specific healthcare regions (p < 0.05) were independently associated with said outcome.
The study highlights, from a systems-level perspective, that there was a significant variation in care pathways and management among the six healthcare regions in Sweden, which might have impacted on clinical outcome. These findings call for more granular studies to understand which aspects of patient management that were particularly beneficial or detrimental for patient survival and recovery.
瑞典国土面积广大,但人口稀少。该国分为六个异质性医疗保健区域,在创伤性脑损伤(TBI)方面,每个区域都有不同的地理条件和转诊模式。本研究旨在探讨该国TBI患者在人口统计学、损伤模式、护理途径、管理及死亡率(30天)方面的差异。
利用瑞典创伤登记处(SweTrau)2018年至2022年的数据进行了一项全国性观察性研究。共纳入5036例TBI患者。评估了人口统计学数据、入院状态(通过首次接诊医院到达时的格拉斯哥昏迷量表[GCS]值)、损伤相关变量及死亡率(30天)。
中位年龄为65岁(四分位间距46 - 78岁),大多数患者为男性,因跌倒受伤,入院时意识清醒。这些变量在各区域之间存在轻微但显著的差异(p < 0.05)。在多变量逻辑回归模型中,在对人口统计学和损伤变量进行调整后,医疗保健区域(p < 0.05)与患者转诊至大学医院(与仅在当地医院接受治疗相比)、开颅率及接受颅内压监测设备独立相关。在关于死亡率的类似回归分析中,特定的医疗保健区域(p < 0.05)与上述结果独立相关。
该研究从系统层面突出表明,瑞典六个医疗保健区域在护理途径和管理方面存在显著差异,这可能对临床结局产生了影响。这些发现需要更细致的研究,以了解患者管理的哪些方面对患者生存和康复特别有益或有害。