Bozkurt Yavuz Hatice, Kutlu Hüseyin Haydar
Department of Clinical Biochemistry, Uşak University Faculty of Medicine, Usak, Turkey.
Department of Medical Microbiology, Uşak University Faculty of Medicine, Usak, Turkey.
Trop Med Int Health. 2025 Aug;30(8):831-837. doi: 10.1111/tmi.14138. Epub 2025 Jun 13.
Crimean-Congo haemorrhagic fever is a lethal tick-borne disease characterised by initially nonspecific symptoms. While thrombocytopenia and leucopenia are established diagnostic markers, there is a need for earlier indicators. This study evaluates lymphopenia as a marker for Crimean-Congo haemorrhagic fever.
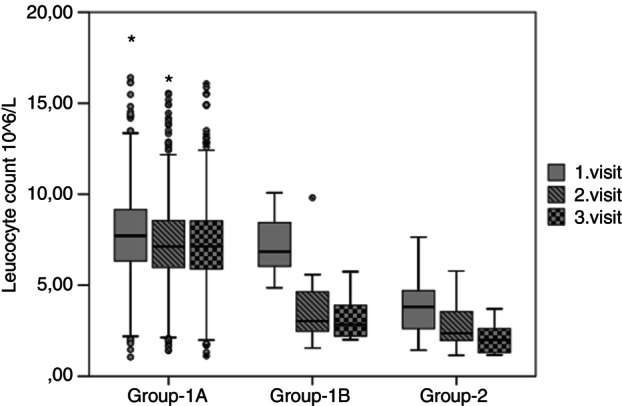
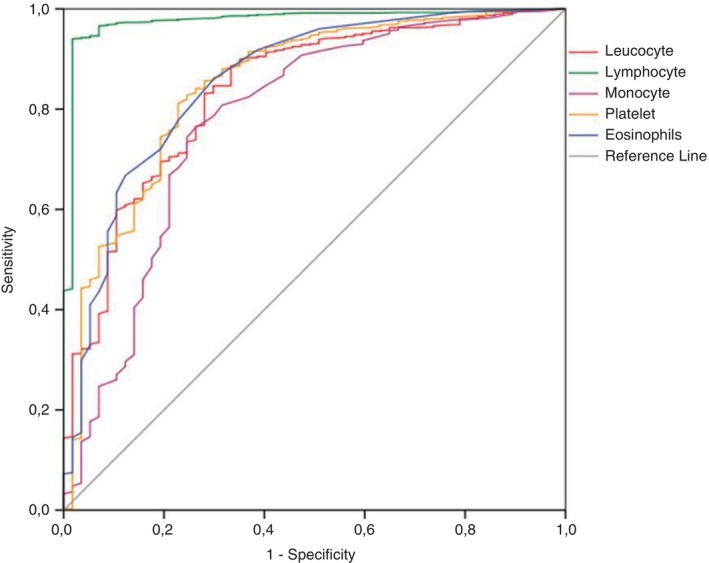
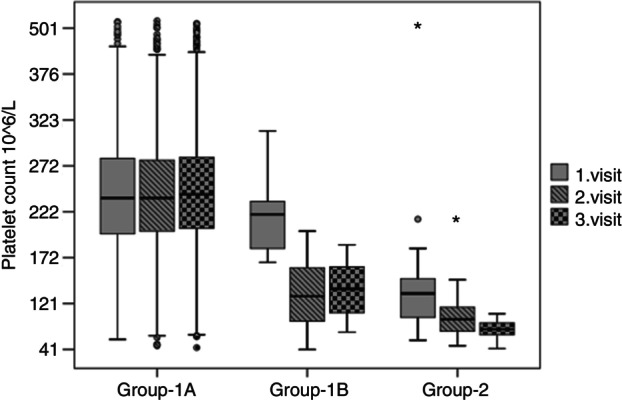
This retrospective study analysed patients admitted with arthropod bites from 2018 to 2021. Patients were classified based on initial leucocyte and platelet counts into Group 1 (normal values) and Group 2 (low values). Within Group 1, patients were classified as Group 1B if they developed thrombocytopenia and leucopenia during follow-up, whereas those with stable counts were designated as Group 1A. Variance and ROC curve analysis were used to evaluate blood counts.
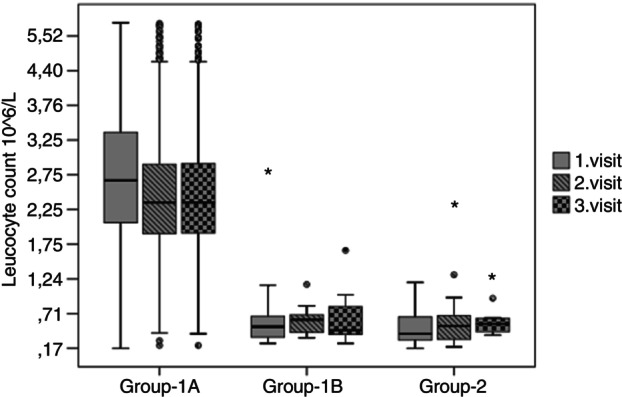
Of 914 evaluated patients, 870 with normal CBCs were categorised into Group 1, and 44 with low counts into Group 2. Within Group 1, 16 patients subsequently developed thrombocytopenia and leucopenia (Group 1B), while the rest remained stable (Group 1A). All patients in Groups 1B and 2 were later confirmed to have Crimean-Congo haemorrhagic fever via RT-PCR. Initial lymphocyte counts varied significantly, with 2.7 × 10/L in Group 1A, 0.52 × 10/L in Group 1B, and 0.42 × 10/L in Group 2, with notable reductions observed in Group 1B and Group 2 (p < 0.001). ROC analysis showed lymphocyte counts below 1.19 × 10/L were the most sensitive and specific for Crimean-Congo haemorrhagic fever (area under curve is 0.976 [95% CI: 0.957-0.995]), exceeding traditional markers.
Lymphocyte depletion precedes changes in leucocyte and platelet counts, affirming its potential as an early diagnostic marker for Crimean-Congo haemorrhagic fever. Early detection through lymphocyte monitoring could improve patient management and reduce transmission in endemic areas.
克里米亚-刚果出血热是一种由蜱传播的致命疾病,初期症状不具特异性。虽然血小板减少和白细胞减少是已确定的诊断标志物,但仍需要更早的指标。本研究评估淋巴细胞减少作为克里米亚-刚果出血热标志物的情况。
这项回顾性研究分析了2018年至2021年因节肢动物叮咬入院的患者。根据初始白细胞和血小板计数将患者分为第1组(正常值)和第2组(低值)。在第1组中,随访期间出现血小板减少和白细胞减少的患者归为1B组,计数稳定的患者归为1A组。采用方差分析和ROC曲线分析来评估血细胞计数。
在914例接受评估的患者中,870例全血细胞计数正常的患者被归入第1组,44例计数低的患者被归入第2组。在第1组中,16例患者随后出现血小板减少和白细胞减少(1B组),其余患者保持稳定(1A组)。1B组和第2组的所有患者后来均通过逆转录聚合酶链反应确诊为克里米亚-刚果出血热。初始淋巴细胞计数差异显著,1A组为2.7×10⁹/L,1B组为0.52×10⁹/L,第2组为0.42×10⁹/L,1B组和第2组均有明显下降(p<0.001)。ROC分析显示,淋巴细胞计数低于1.19×10⁹/L对克里米亚-刚果出血热最为敏感和特异(曲线下面积为0.976[95%CI:0.957 - 0.995]),超过了传统标志物。
淋巴细胞减少先于白细胞和血小板计数的变化,证实了其作为克里米亚-刚果出血热早期诊断标志物的潜力。通过淋巴细胞监测进行早期检测可改善患者管理并减少流行地区的传播。