Singer Cristina Elena, Popescu Cristina, Trasca Diana-Maria, Varut Renata-Maria, Serban Rebecca-Cristiana, Abdul-Razzak Jaqueline, Radulescu Virginia-Maria
Department of Mother and Baby, University of Medicine and Pharmacy of Craiova, 200349 Craiova, Romania.
Department of Anatomy, University of Medicine and Pharmacy, Discipline of Anatomy, 200349 Craiova, Romania.
Children (Basel). 2025 Jun 9;12(6):746. doi: 10.3390/children12060746.
BACKGROUND/OBJECTIVES: Neonatal and infant respiratory distress carries high morbidity, and severity can vary with gestational maturity and perinatal factors. Early risk stratification may improve outcomes, but existing assessment tools do not fully address age-related risk differences. We aimed to develop and validate a Neonatal Clinical Risk Assessment Score (N-CRAS) for predicting severity in neonates and young infants with respiratory distress due to respiratory infection.
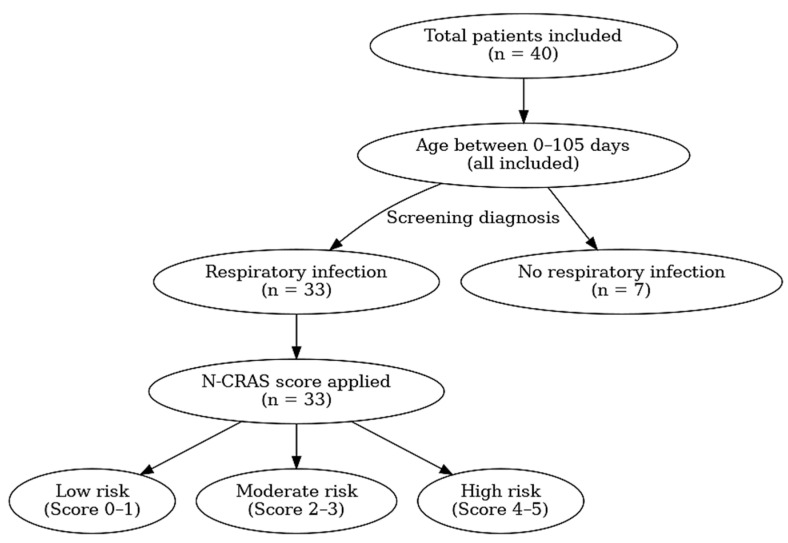
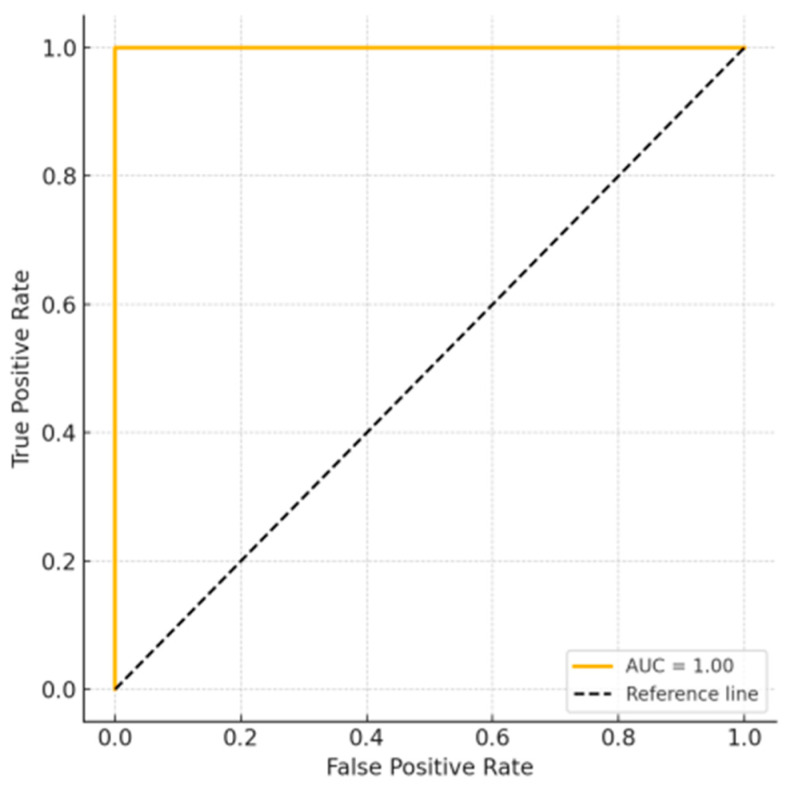
This pilot score was applied exclusively to a cohort of forty neonates and young infants with respiratory distress secondary to infectious causes, as defined by clinical and laboratory parameters. Clinical variables (gestational age, delivery mode, birth weight category, and APGAR score) were recorded and analyzed for associations with illness severity. We developed the N-CRAS (0-5 points) encompassing five indicators of severe illness (respiratory infection, metabolic disorder, need for symptomatic treatment, mechanical ventilation, and intubation), each contributing 1 point. Patients were stratified as low (0-1), moderate (2-3), or high (4-5) risk. Chi-square tests and Spearman correlation assessed associations, and an ROC curve evaluated the score's predictive performance for intubation.
No individual perinatal factor was significantly associated with respiratory illness severity. The N-CRAS increased with infant age ( < 0.05), indicating older infants tended to have more severe disease. All study infants who required intubation fell into the high-risk category (score ≥ 4). The N-CRAS demonstrated excellent discrimination for predicting intubation (ROC area under the curve = 1.00).
In this pilot study, the N-CRAS demonstrated a strong correlation with clinical severity and successfully identified all infants who required intubation. However, given the small cohort size and limited number of severe cases, these findings should be interpreted cautiously. Further external validation in larger and more diverse neonatal populations is essential to confirm its predictive utility.
背景/目的:新生儿和婴儿呼吸窘迫发病率高,其严重程度会因胎龄和围产期因素而有所不同。早期风险分层可能会改善预后,但现有的评估工具并未充分考虑与年龄相关的风险差异。我们旨在开发并验证一种新生儿临床风险评估评分(N-CRAS),用于预测因呼吸道感染导致呼吸窘迫的新生儿和幼儿的病情严重程度。
该初步评分仅应用于一组40例因感染性原因导致呼吸窘迫的新生儿和幼儿,其由临床和实验室参数定义。记录并分析临床变量(胎龄、分娩方式、出生体重类别和阿氏评分)与疾病严重程度的相关性。我们开发了包含五个严重疾病指标(呼吸道感染、代谢紊乱、对症治疗需求、机械通气和插管)的N-CRAS(0至5分),每个指标计1分。将患者分为低风险(0至1分)、中度风险(2至3分)或高风险(4至5分)。采用卡方检验和斯皮尔曼相关性评估相关性,并用ROC曲线评估该评分对插管的预测性能。
没有单个围产期因素与呼吸道疾病严重程度显著相关。N-CRAS随婴儿年龄增加而升高(<0.05),表明年龄较大的婴儿往往病情更严重。所有需要插管的研究婴儿均属于高风险类别(评分≥4分)。N-CRAS在预测插管方面表现出出色的辨别能力(曲线下面积=1.00)。
在这项初步研究中,N-CRAS与临床严重程度显示出强相关性,并成功识别出所有需要插管的婴儿。然而,鉴于样本量小且严重病例数量有限,这些发现应谨慎解读。在更大且更多样化的新生儿群体中进行进一步的外部验证对于确认其预测效用至关重要。