Virdun Claudia, Singh Gursharan K, Yates Patsy, Phillips Jane L, Mudge Alison
Palliative & End of Life Care, College of Nursing and Health Sciences, and member, Flinders Research Centre for Palliative Care, Death, and Dying, Flinders University, Adelaide, SA, Australia.
Cancer and Palliative Care Outcomes Centre, Centre for Healthcare Transformation, Faculty of Health, Queensland University of Technology (QUT), Brisbane, QLD, Australia.
BMC Palliat Care. 2025 Jul 2;24(1):185. doi: 10.1186/s12904-025-01815-1.
Population ageing and rising levels of non-communicable diseases are increasing the number of people living with and dying from advanced serious illnesses globally. Many of these people are hospitalised more than once in their last year of life. While there is sound evidence on what patients and their families require for safe and high-quality hospital palliative care, enabling this remains a challenge. This study aimed to understand the clinician, team, and organisational-level barriers and enablers to integrating good palliative care into acute care.
An exploratory-descriptive, qualitative study involving semi-structured interviews and practical thematic analysis was conducted. Medical, nursing and allied health disciplines were recruited from three wards (cancer care, mixed general medicine/renal and mixed general medicine/respiratory) within a large Australian metropolitan hospital.
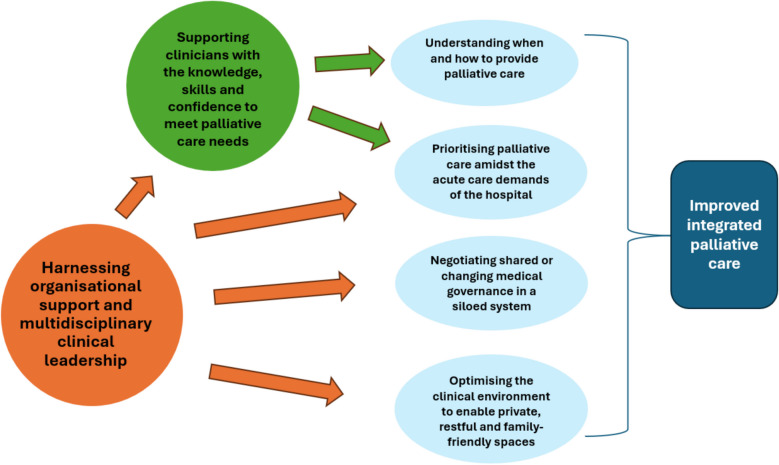
Eighty-eight interviews (nursing (n = 39); medicine (n = 24); allied health (n = 25)) were undertaken, with a median duration of 25.5 min (range 5 to 55 min). Most participants were female (n = 73, 83%), holding a Bachelor's degree (n = 86, 98%) and ranged from new graduates to participants with over 40 years of post-registration experience. The analysis generated six themes, reflecting the challenges of providing optimal palliative care within acute hospital wards: 1. Understanding when and how to provide palliative care 2. Negotiating shared or changing medical governance in a siloed system 3. Supporting clinicians with the knowledge, skills and confidence to meet palliative care needs 4. Prioritising palliative care amidst the acute care demands of the hospital 5. Optimising the clinical environment to enable private, restful and family-friendly spaces 6. Harnessing organisational support and multidisciplinary clinical leadership CONCLUSIONS: This study reveals complex, multi-level organisational barriers to integrating palliative care within the acute hospital which will need to be addressed for effective and sustained improvement. Harnessing organisational support and multidisciplinary clinical leadership is key to successful change. Improvements with a focus on developing clinician knowledge, skills, and confidence in palliative care need to pay attention to organisational siloes that constrain shared care, cultures of care that prioritise cure and efficiency, clinical uncertainty in the context of advanced serious illness and optimising the environment for quality palliative care.
全球人口老龄化以及非传染性疾病水平的上升,使得罹患晚期重症并因此死亡的人数不断增加。这些人中许多在生命的最后一年会多次住院。尽管有充分证据表明患者及其家人对安全且高质量的医院姑息治疗有何需求,但要实现这一点仍是一项挑战。本研究旨在了解将优质姑息治疗融入急性护理在临床医生、团队及组织层面所面临的障碍和促成因素。
开展了一项探索性描述性定性研究,包括半结构化访谈和实用主题分析。从澳大利亚一家大型都市医院的三个病房(癌症护理、综合内科/肾脏科混合病房以及综合内科/呼吸科混合病房)招募了医学、护理和专职医疗学科的人员。
共进行了88次访谈(护理人员39名;医生24名;专职医疗人员25名),访谈时长中位数为25.5分钟(范围为5至55分钟)。大多数参与者为女性(73名,83%),拥有本科学历(86名,98%),涵盖从新毕业生到注册后有40多年工作经验的人员。分析得出六个主题,反映了在急性医院病房提供最佳姑息治疗所面临的挑战:1. 了解何时以及如何提供姑息治疗;2. 在孤立的系统中协商共享或变化的医疗管理;3. 为临床医生提供满足姑息治疗需求的知识、技能和信心支持;4. 在医院急性护理需求中优先考虑姑息治疗;5. 优化临床环境以营造私密、宁静且利于家庭的空间;6. 利用组织支持和多学科临床领导力。
本研究揭示了在急性医院中整合姑息治疗存在复杂的多层次组织障碍,要实现有效且持续的改善,必须解决这些障碍。利用组织支持和多学科临床领导力是成功变革的关键。在关注培养临床医生在姑息治疗方面的知识、技能和信心时,改进措施需要关注限制共享护理的组织孤岛、优先考虑治愈和效率的护理文化、晚期重症背景下的临床不确定性以及优化优质姑息治疗的环境。