Ahmadi Shad Maryam, Khorasanizadeh MohammadHossein, Musy Sarah N, Zúñiga Franziska, Atoof Fatemeh, Simon Michael
Institute of Nursing Science, Department of Public Health, University of Basel, Switzerland.
Trauma Nursing Research Center, Kashan University of Medical Sciences, Kashan, Iran.
Int J Nurs Stud Adv. 2025 Jul 16;9:100383. doi: 10.1016/j.ijnsa.2025.100383. eCollection 2025 Dec.
Hospitals deploy temporary nurses to bridge staffing gaps. However, evidence remains inconclusive regarding the extent, patterns, and factors driving temporary deployment. This study aimed to describe how temporary nurses are deployed as a response to shift-level schedule deviations and shortfalls in planned schedules.
Our four-month time-series analysis covered 1344 shifts across two medical and two surgical units in a tertiary hospital in Iran. Shift-level data included nursing staff numbers, the skill mix, staff absences and the patient count and turnover. The patient-to-nurse ratio was used to gauge staffing levels. Data were analysed using both descriptive and analytical approaches, including the fitting of three generalized linear mixed models to assess potential drivers of shifts involving temporary RNs.
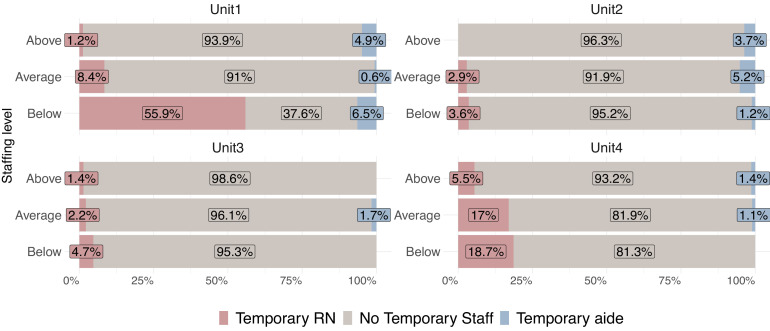
Temporary nurses worked on 12.2 % of shifts with the majority being Registered Nurses (RNs) (81.7 %). Only 28.5 % of deviations led to temporary RN deployments. While students and aides were sometimes reallocated to fill absences, the majority of absences (57.1 %) went unaddressed. Temporary staff mainly worked on shifts with below-average RN-staffing. Unit-level deployment rates varied widely (3.6 %-55.9 %). Model 1 revealed that RN absence increased the odds of using a temporary RN by 2.14 times (AIC = 785.1). Model 2 indicated that each additional patient, increased the odds by 11 % (AIC = 740.7). Model 3 showed that when RN-staffing was below-average the odds of using a temporary RN were 3.96 times higher than the average level (AIC = 707.4).
Temporary nurse deployment was relatively infrequent. While temporary nurses were strategically deployed to address understaffing and short-notice deviations, their deployment did not fully bridge the staffing needs. On high-demand units, temporary staff were commonly supplemented by reallocating students. Some temporary deployments occurred even where RN-staffing was at an average level. These findings indicate an urgent need to enhance the effectiveness of temporary deployment and optimize workforce resources to ensure high-quality care.
医院会部署临时护士以填补人员配备缺口。然而,关于临时部署的程度、模式和驱动因素的证据仍不确凿。本研究旨在描述临时护士是如何作为对班次级排班偏差和计划排班不足的应对措施而进行部署的。
我们为期四个月的时间序列分析涵盖了伊朗一家三级医院两个内科和两个外科科室的1344个班次。班次级数据包括护理人员数量、技能组合、员工缺勤情况以及患者数量和周转率。患者与护士的比例用于衡量人员配备水平。数据采用描述性和分析性方法进行分析,包括拟合三个广义线性混合模型,以评估涉及临时注册护士的班次的潜在驱动因素。
临时护士参与了12.2%的班次,其中大多数是注册护士(81.7%)。只有28.5%的偏差导致了临时注册护士的部署。虽然有时会重新分配学生和助手来填补缺勤,但大多数缺勤(57.1%)未得到解决。临时工作人员主要在注册护士配备低于平均水平的班次工作。科室层面的部署率差异很大(3.6%-55.9%)。模型1显示,注册护士缺勤使使用临时注册护士的几率增加了2.14倍(AIC = 785.1)。模型2表明,每增加一名患者,几率增加11%(AIC = 740.7)。模型3显示,当注册护士配备低于平均水平时,使用临时注册护士的几率比平均水平高3.96倍(AIC = 707.4)。
临时护士的部署相对较少。虽然临时护士是为解决人员短缺和临时偏差而进行战略部署的,但其部署并未完全满足人员配备需求。在高需求科室,通常通过重新分配学生来补充临时工作人员。即使在注册护士配备处于平均水平的情况下,也会有一些临时部署。这些发现表明迫切需要提高临时部署的有效性并优化劳动力资源,以确保高质量护理。