Orloff M J, Johansen K H
Ann Surg. 1978 Oct;188(4):494-512. doi: 10.1097/00000658-197810000-00007.
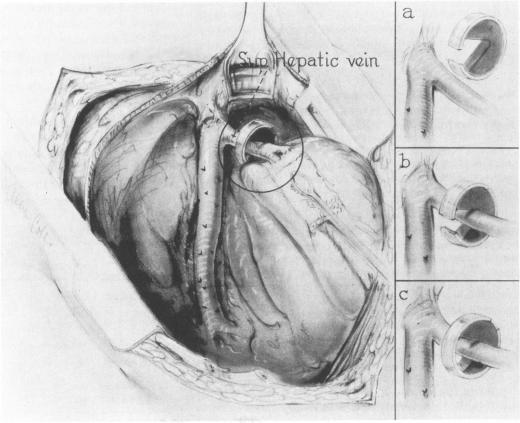
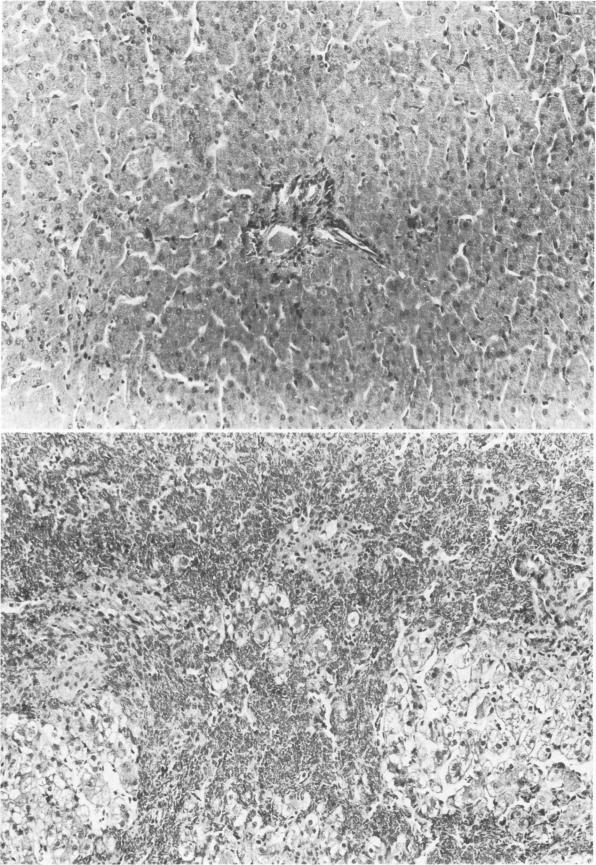
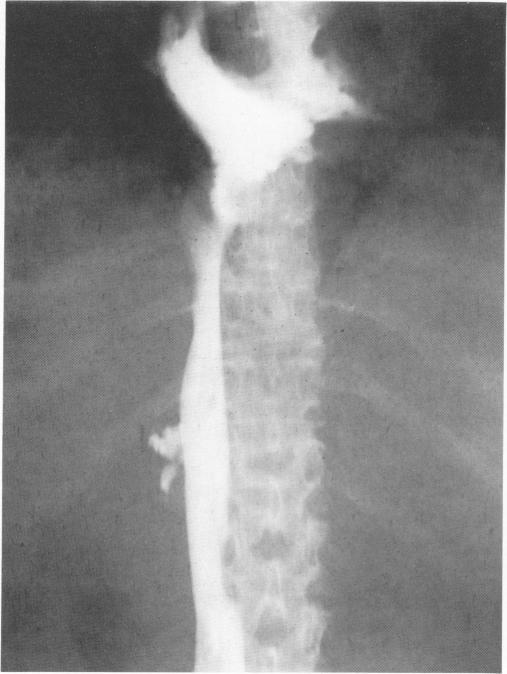
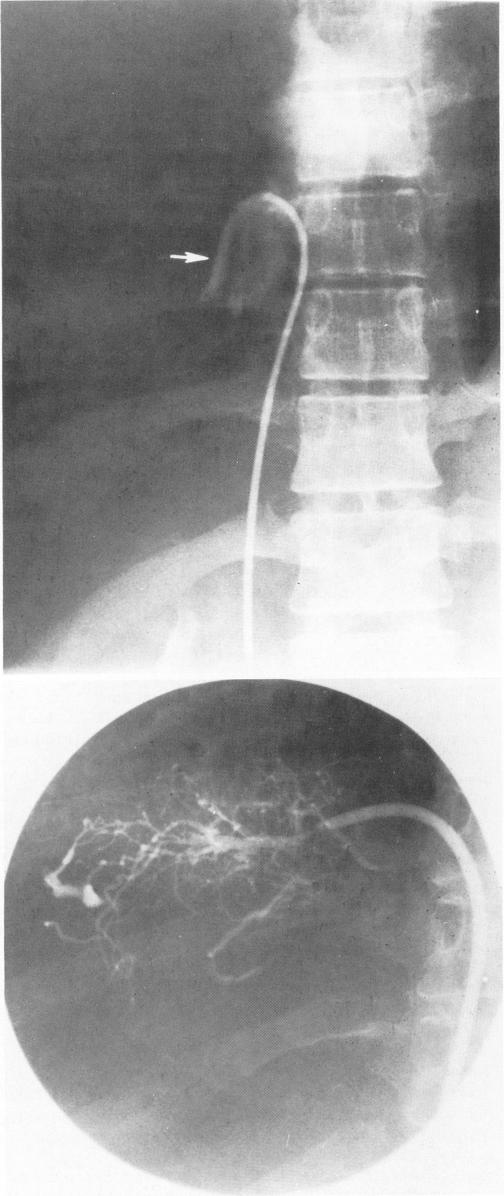
The Budd-Chiari syndrome caused by occlusion of the major hepatic veins, often of unknown etiology, is typically characterized by massive ascites, hepatomegaly and abdominal pain due to intense congestion of the liver. The outcome has almost always been fatal. This report describes an evaluation of side-to-side portacaval shunt in dogs with experimental Budd-Chiari syndrome and in six patients with hepatic vein thrombosis. In the animal studies, side-to-side portacaval shunt was very effective in relieving massive ascites, hepatomegaly, hepatic congestion and portal hypertension produced by ligation of the hepatic veins. Only one of 24 dogs with side-to-side anastomosis reformed ascites, 67% of the animals survived until the study was concluded after one year, and liver biopsies showed reversal of the severe pathologic abnormalities. In contrast, all 20 control dogs subjected to a sham laparotomy, and all 20 dogs that underwent end-to-side portacaval shunt reformed massive ascites and died within six months with continued hepatic congestion and necrosis. All six patients with the Budd-Chiari syndrome due to hepatic vein occlusion had massive ascites (4.4-15.9 l), hepatomegaly, abdominal pain and disturbed liver function. In all six, angiography demonstrated occlusion of the hepatic veins with a patent inferior vena cava (IVC) and a normal IVC pressure, and liver biopsy showed intense centrilobular congestion and necrosis. The most valuable diagnostic study was angiography of the IVC and hepatic veins with pressure measurements. Side-to-side portacaval shunt was performed from four to 14 weeks after the onset of symptoms, and produced dramatic and sustained relief of ascites in five of the six patients during follow-up periods of from eight months to seven years. Liver function returned to normal, hepatosplenomegaly disappeared, none of the survivors developed portal-systemic encephalopathy, and follow-up liver biopsies showed disappearance of congestion and necrosis, but mild to moderate fibrosis. One patient died following an emergency IVC thrombectomy and portacaval shunt, which was undertaken when, during the course of his workup, his condition deteriorated suddenly because the thrombotic process extended from the hepatic veins into the IVC. The everpresent risk of this complication, and the dangers associated with delaying operation were emphasized by this case. It is concluded that side-to-side portacaval shunt, which decompresses the liver by converting the portal vein into an outflow tract, provides effective treatment of the Budd-Chiari syndrome when the occlusive process is confined to the hepatic veins.
布加综合征由主要肝静脉闭塞引起,病因通常不明,其典型特征为因肝脏严重充血而出现大量腹水、肝肿大和腹痛。其预后几乎总是致命的。本报告描述了对患有实验性布加综合征的犬以及6例肝静脉血栓形成患者进行侧侧门腔分流术的评估。在动物研究中,侧侧门腔分流术对于缓解因结扎肝静脉而产生的大量腹水、肝肿大、肝脏充血和门静脉高压非常有效。在24只接受侧侧吻合术的犬中,只有1只再次出现腹水,67%的动物存活至一年后研究结束,肝脏活检显示严重病理异常得到逆转。相比之下,所有20只接受假剖腹手术的对照犬以及所有20只接受端侧门腔分流术的犬均再次出现大量腹水,并在6个月内死亡,伴有持续的肝脏充血和坏死。所有6例因肝静脉闭塞导致布加综合征的患者均有大量腹水(4.4 - 15.9升)、肝肿大、腹痛和肝功能紊乱。在所有6例患者中,血管造影显示肝静脉闭塞,下腔静脉通畅且下腔静脉压力正常,肝脏活检显示严重的小叶中心充血和坏死。最有价值的诊断检查是下腔静脉和肝静脉血管造影及压力测量。侧侧门腔分流术在症状出现后4至14周进行,在6例患者中的5例随访8个月至7年期间,腹水得到显著且持续的缓解。肝功能恢复正常,肝脾肿大消失,所有存活者均未发生门体性脑病,随访肝脏活检显示充血和坏死消失,但有轻度至中度纤维化。1例患者在检查过程中病情突然恶化,因为血栓形成过程从肝静脉扩展至下腔静脉,随后进行了紧急下腔静脉血栓切除术和门腔分流术,术后死亡。该病例强调了这种并发症始终存在的风险以及延迟手术的危险性。结论是,当闭塞过程局限于肝静脉时,通过将门静脉转变为流出道来减轻肝脏压力的侧侧门腔分流术可有效治疗布加综合征。