Leigh T R, Gazzard B G, Rowbottom A, Collins J V
Department of Respiratory Medicine, Westminster Hospital, London.
J Clin Pathol. 1993 Feb;46(2):140-4. doi: 10.1136/jcp.46.2.140.
To compare the results of DNA amplification by the polymerase chain reaction (PCR) with immunofluorescence staining for detecting Pneumocystis carinii in bronchoalveolar lavage specimens taken from symptomatic HIV seropositive patients with suspected P carinii pneumonia (PCP).
Bronchoalveolar lavage specimens were obtained from 28 symptomatic HIV seropositive patients. Specimens were examined for P carinii using immunofluorescence, and by DNA amplification with PCR to obtain results on gel electrophoresis (gel) and a more sensitive Southern hybridisation (blot) technique. Specimens positive by immunofluorescence and gel electrophoresis were serially diluted to a 10(-6) concentration and each dilution strength tested for P carinii using PCR to compare quantitatively immunofluorescence with PCR.
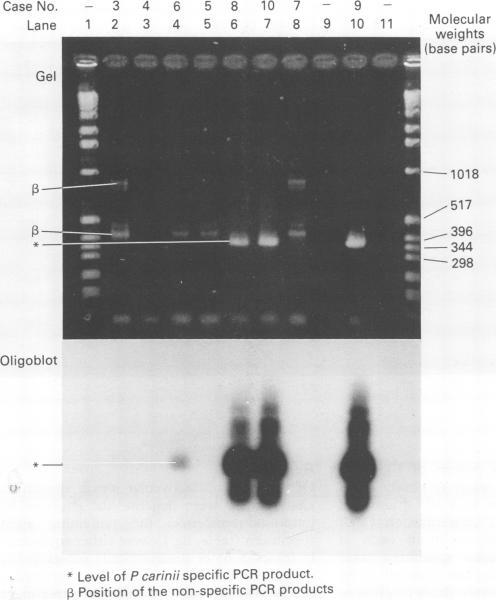
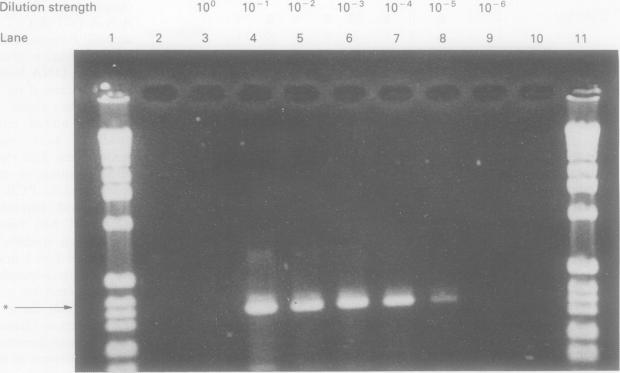
Of the 28 specimens analysed, 18 were negative for P carinii by both immunofluorescence and PCR, two were positive only by the blot technique of PCR, four were equivocally positive and four unequivocally positive by immunofluorescence. Three of the four equivocally positive patients tested by immunofluorescence were negative for P carinii by PCR, although one was positive by PCR (blot) technique. This patient had clinically confirmed PCP. Of the four unequivocally positive patients tested by immunofluorescence, three were gel and blot positive by PCR and had PCP clinically, but one was negative by both gel and blot techniques, although the patient certainly had PCP on clinical grounds. This patient had received nine days of treatment with high dose co-trimoxazole before bronchoalveolar lavage specimens were obtained. The three specimens positive by gel and blot techniques remained gel positive down to dilutions of between 10(-4) and 10(-6).
PCR results may become negative soon after starting treatment for PCP. Specimens should therefore be taken before, or soon after, starting treatment. PCR seems to be between 10(4) and 10(6) times more sensitive than immunofluorescence.
比较聚合酶链反应(PCR)进行DNA扩增与免疫荧光染色检测有症状的疑似卡氏肺孢子虫肺炎(PCP)的HIV血清阳性患者支气管肺泡灌洗标本中卡氏肺孢子虫的结果。
从28例有症状的HIV血清阳性患者获取支气管肺泡灌洗标本。采用免疫荧光法检测标本中的卡氏肺孢子虫,并通过PCR进行DNA扩增,以获得凝胶电泳(凝胶)和更敏感的Southern杂交(印迹)技术的结果。将免疫荧光和凝胶电泳阳性的标本连续稀释至10⁻⁶浓度,并用PCR检测各稀释度的卡氏肺孢子虫,以定量比较免疫荧光与PCR。
在分析的28个标本中,18个通过免疫荧光和PCR检测卡氏肺孢子虫均为阴性,2个仅通过PCR的印迹技术呈阳性,4个为可疑阳性,4个通过免疫荧光明确为阳性。免疫荧光检测为可疑阳性的4例患者中,3例PCR检测卡氏肺孢子虫为阴性,尽管1例通过PCR(印迹)技术呈阳性。该患者临床确诊为PCP。免疫荧光检测为明确阳性的4例患者中,3例PCR凝胶和印迹均呈阳性且临床诊断为PCP,但1例凝胶和印迹技术均为阴性,尽管该患者临床确诊为PCP。该患者在获取支气管肺泡灌洗标本前已接受9天高剂量复方新诺明治疗。凝胶和印迹技术呈阳性的3个标本在稀释至10⁻⁴至10⁻⁶之间时仍为凝胶阳性。
PCP治疗开始后不久PCR结果可能转阴。因此,标本应在治疗开始前或开始后不久采集。PCR的敏感性似乎比免疫荧光高10⁴至10⁶倍。