Niemelä S, Karttunen T, Kerola T, Karttunen R
Department of Internal Medicine, University Hospital of Oulu, Finland.
J Clin Pathol. 1995 Dec;48(12):1111-6. doi: 10.1136/jcp.48.12.1111.
To examine the course of lymphocytic gastritis and its relation to Helicobacter pylori (H pylori) infection in a 10 year follow up.
Ninety six patients were originally examined for dyspepsia in 1981. Gastroscopies with stepwise biopsies were performed on all the patients initially and after an interval of 10 years.
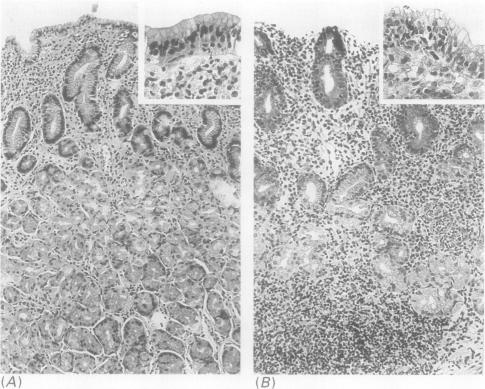
Nine per cent of the patients (9/96) had features of lymphocytic gastritis in gastric biopsy at the first examination, and 12.5% (12/96) at the second examination; 7/9 patients (78%) had persistent lymphocytic gastritis during the follow up; in two the diagnostic features of lymphocytic gastritis had disappeared, and five had a new diagnosis of lymphocytic gastritis at the second examination. At the second examination 9/12 lymphocytic gastritis patients (75%) were H pylori positive histologically, while all had specific antibodies to H pylori. The lymphocytic gastritis patients had higher grades of gastritis (p = 0.009), neutrophilic and eosinophilic granulocytes, mononuclear inflammatory cells, and foveolar hyperplasia in the corpus mucosa, but smaller numbers of H pylori, than the H pylori positive patients without lymphocytic gastritis. The appearance of lymphocytic gastritis during the 10 year interval was associated with increases in the grades of corpus gastritis and neutrophilic granulocytes (p = 0.043 for both). During the follow up, the patients with lymphocytic gastritis, but not the H pylori positive patients without lymphocytic gastritis, appeared to have a significant increase in the grade of intestinal metaplasia in the corpus mucosa (p = 0.043).
In some patients H pylori may cause a gastritis that predominates in the corpus and is associated with an increase in the intraepithelial lymphocyte count. This form of gastritis may cause progression of intestinal metaplasia.
通过10年随访研究淋巴细胞性胃炎的病程及其与幽门螺杆菌(H pylori)感染的关系。
1981年对96例因消化不良就诊的患者进行了初步检查。所有患者最初均接受了胃镜检查及逐步活检,并在10年后再次进行检查。
首次检查时,9%(9/96)的患者胃活检显示有淋巴细胞性胃炎特征,第二次检查时为12.5%(12/96);随访期间,9例患者中有7例(78%)持续性淋巴细胞性胃炎;2例淋巴细胞性胃炎的诊断特征消失,5例在第二次检查时新诊断为淋巴细胞性胃炎。第二次检查时,12例淋巴细胞性胃炎患者中有9例(75%)组织学检查显示幽门螺杆菌阳性,而所有患者均有幽门螺杆菌特异性抗体。与无淋巴细胞性胃炎的幽门螺杆菌阳性患者相比,淋巴细胞性胃炎患者的胃炎分级更高(p = 0.009),胃体黏膜中的中性粒细胞、嗜酸性粒细胞、单核炎性细胞及小凹增生更明显,但幽门螺杆菌数量更少。10年间淋巴细胞性胃炎的出现与胃体胃炎分级及中性粒细胞增加有关(两者p值均为0.043)。随访期间,有淋巴细胞性胃炎的患者,而非无淋巴细胞性胃炎的幽门螺杆菌阳性患者,胃体黏膜肠化生分级似乎有显著增加(p = 0.043)。
在一些患者中,幽门螺杆菌可能引起以胃体为主的胃炎,并伴有上皮内淋巴细胞计数增加。这种胃炎形式可能导致肠化生进展。