Schaberg T, Gialdroni-Grassi G, Huchon G, Leophonte P, Manresa F, Woodhead M
Pulmonary Section, Chest Clinic Zum, Berlin, Germany.
Thorax. 1996 Oct;51(10):1017-22. doi: 10.1136/thx.51.10.1017.
The purpose of this study was to identify factors on which European general practitioners (GPs) base their decisions to admit to hospital patients with lower respiratory tract infections (LRTI).
A survey was carried out from December 1993 to January 1994 to identify factors that affect GPs' decisions to admit to hospital patients with LRTI by collecting data on 2056 patients from 605 GPs in France, Germany, Italy, Spain, and the UK.
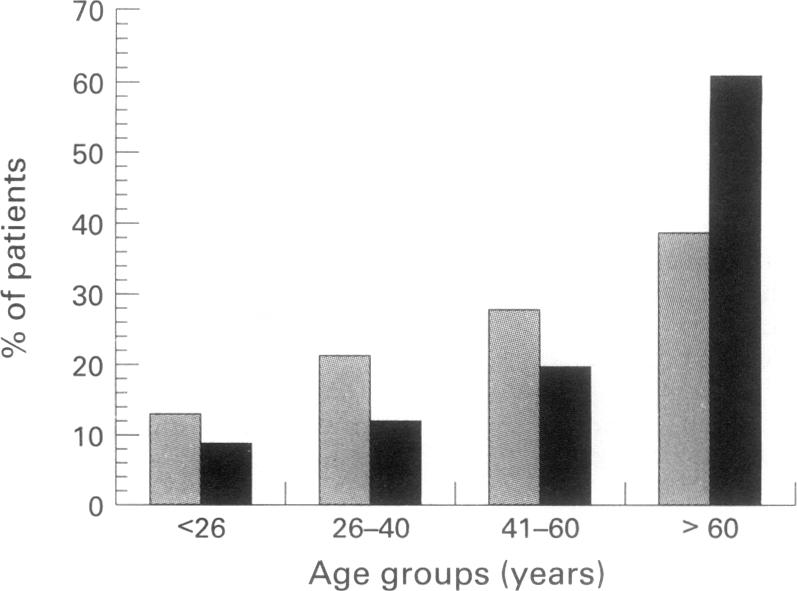
Only 93 (4.5%) of the patients included in the study were admitted to hospital. Univariate analysis showed that age > 60 years, institutionalisation of the patient, concomitant diseases, cardiac insufficiency, asthma, a diagnosis of pneumonia, and clinical signs such as chest pain, cyanosis, tachypnoea and hypotension significantly (odds ratio (OR) > 2.0, p < 0.002) influenced the decision to admit to hospital. No influence could be shown for sex, smoking habits, history of bronchiectasis or chronic bronchitis, the presence of fever, chills, myalgia, cough or purulent sputum, and the diagnoses of acute bronchitis, influenza or exacerbation of chronic bronchitis. In the multivariate analysis only the presence of chest pain (OR 2.3, 95% confidence interval (CI) 1.5 to 3.5), cyanosis (OR 4.1, 95% CI 2.4 to 7.1), dyspnoea (OR 4.9, 95% CI 3.1 to 7.9), and hypotension (OR 2.9, 95% CI 1.6 to 5.2), as well as a diagnosis of pneumonia (OR 6.6, 95% CI 4.3 to 10) (all p < 0.00001) remained as factors that significantly affected the decision to admit to hospital.
Clinical signs of severe infection and a diagnosis of pneumonia are the main factors that induce GPs to admit patients with LRTI to hospital in Europe.
本研究旨在确定欧洲全科医生(GP)决定收治下呼吸道感染(LRTI)患者时所依据的因素。
于1993年12月至1994年1月开展了一项调查,通过收集来自法国、德国、意大利、西班牙和英国605名全科医生的2056例患者的数据,来确定影响全科医生收治下呼吸道感染患者决策的因素。
纳入研究的患者中仅有93例(4.5%)被收治入院。单因素分析显示,年龄>60岁、患者入住养老院、合并症、心功能不全、哮喘、肺炎诊断以及胸痛、发绀、呼吸急促和低血压等临床体征对收治决策有显著影响(比值比(OR)>2.0,p<0.002)。性别、吸烟习惯、支气管扩张或慢性支气管炎病史、发热、寒战、肌痛、咳嗽或脓性痰的存在以及急性支气管炎、流感或慢性支气管炎急性加重的诊断未显示出有影响。多因素分析中,只有胸痛(OR 2.3,95%置信区间(CI)1.5至3.5)、发绀(OR 4.1,95%CI 2.4至7.1)、呼吸困难(OR 4.9,95%CI 3.1至7.9)、低血压(OR 2.9,95%CI 1.6至5.2)以及肺炎诊断(OR 6.6,95%CI 4.3至10)(所有p<0.00001)仍是显著影响收治决策的因素。
严重感染的临床体征和肺炎诊断是欧洲全科医生收治下呼吸道感染患者入院的主要因素。