Watters J M, Kirkpatrick S M, Norris S B, Shamji F M, Wells G A
Department of Surgery, University of Ottawa, and Ottawa Civic Hospital, Ontario, Canada.
Ann Surg. 1997 Sep;226(3):369-77; discussion 377-80. doi: 10.1097/00000658-199709000-00016.
The authors set out to determine whether immediate enteral feeding minimizes early postoperative decreases in handgrip and respiratory muscle strength.
Muscle strength decreases considerably after major surgical procedures. Enteral feeding has been shown to restore strength rapidly in other clinical settings.
A randomized, controlled, nonblinded clinical trial was conducted in patients undergoing esophagectomy or pancreatoduodenectomy who received immediate postoperative enteral feeding via jejunostomy (fed, n = 13), or no enteral feeding during the first 6 postoperative days (unfed, n = 15). Handgrip strength, vital capacity, forced expiratory volume in one second (FEV1), and maximal inspiratory pressure (MIP) were measured before surgery and on postoperative days 2, 4, and 6. Fatigue and vigor were evaluated before surgery and on postoperative day 6. Mobility was assessed daily after surgery using a standardized descriptive scale. Postoperative urine biochemistry was evaluated in daily 24-hour collections.
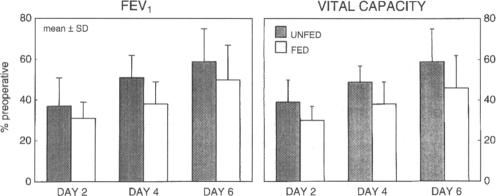
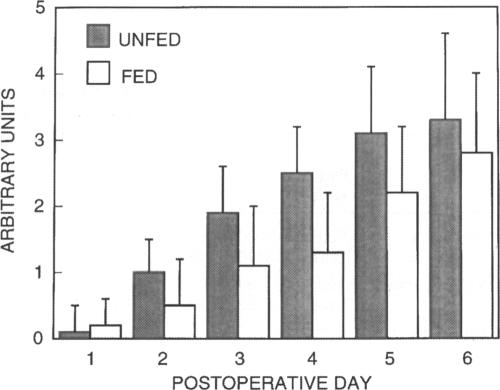
Postoperative vital capacity (p < 0.05) and FEV1 (p = 0.07) were consistently lower (18%-29%) in the fed group than in the unfed group, whereas grip strength and maximal inspiratory pressure were not significantly different. Postoperative mobility also was lower in the fed patients (p < 0.05) and tended to recover less rapidly (p = 0.07). Fatigue increased and vigor decreased after surgery (both p < or = 0.001), but changes were similar in the fed and unfed groups. Intensive care unit and postoperative hospital stay did not differ between groups.
Immediate postoperative jejunal feeding was associated with impaired respiratory mechanics and postoperative mobility and did not influence the loss of muscle strength or the increase in fatigue, which occurred after major surgery. Immediate postoperative enteral feeding should not be routine in well-nourished patients at low risk of nutrition-related complications.
作者旨在确定术后立即肠内喂养是否能将术后早期握力和呼吸肌力量的下降降至最低。
大手术后肌肉力量会显著下降。在其他临床环境中,肠内喂养已被证明能迅速恢复力量。
对接受食管切除术或胰十二指肠切除术的患者进行了一项随机、对照、非盲临床试验,这些患者术后立即通过空肠造口术接受肠内喂养(喂养组,n = 13),或在术后第1至6天不接受肠内喂养(未喂养组,n = 15)。在手术前以及术后第2、4和6天测量握力、肺活量、一秒用力呼气量(FEV1)和最大吸气压力(MIP)。在手术前和术后第6天评估疲劳和活力。术后每天使用标准化描述量表评估活动能力。术后每天收集24小时尿液进行生化评估。
喂养组术后肺活量(p < 0.05)和FEV1(p = 0.07)始终比未喂养组低(18% - 29%),而握力和最大吸气压力无显著差异。喂养组患者术后活动能力也较低(p < 0.05),且恢复速度往往较慢(p = 0.07)。手术后疲劳增加,活力下降(均p ≤ 0.001),但喂养组和未喂养组的变化相似。两组之间重症监护病房停留时间和术后住院时间无差异。
术后立即空肠喂养与呼吸力学受损和术后活动能力下降有关,且不影响大手术后发生的肌肉力量丧失或疲劳增加。对于营养相关并发症风险较低的营养良好患者,术后立即肠内喂养不应作为常规操作。