Department of Medical Oncology and Hematology, Istituto Clinico Humanitas Rozzano (MI), Italy.
Ther Clin Risk Manag. 2006 Sep;2(3):229-34. doi: 10.2147/tcrm.2006.2.3.229.
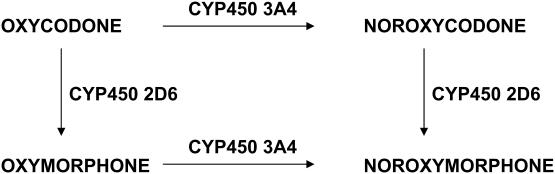
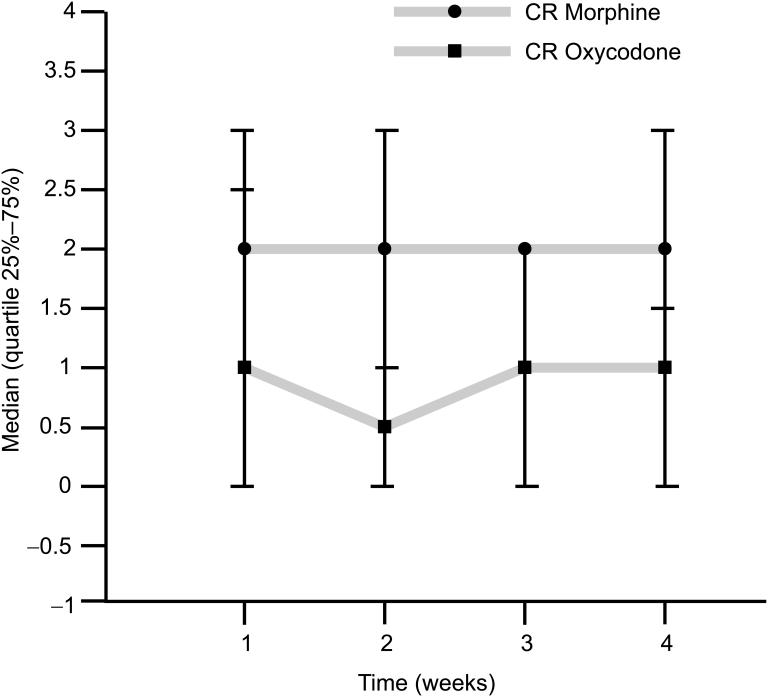
Oral opioids are the treatment of choice for chronic cancer pain. Morphine is the strong opioid of choice for the treatment of moderate to severe cancer pain according to guidelines from the World Health Organization (WHO). This recommendation by the WHO was derived from availability, familiarity to clinicians, established effectiveness, simplicity of administration, and relative inexpensive cost. It was not based on proven therapeutic superiority over other options. Patients who experience inadequate pain relief or intolerable side effects with one opioid may often be successfully treated with another agent or with the same agent administered by a different route. Opioid rotation, or switching to an alternative opioid, helps some patients achieve better pain control with fewer associated adverse effects. Oxycodone is a mu-opioid receptor specific ligand, with clear agonist properties. It is an active potent opioid, which is in part a kappa-receptor agonist. Like morphine and other pure agonists, there is no known ceiling to the analgesic effects of oxycodone. The active metabolites of oxycodone (eg, oxymorphone) could be important in oxycodone-mediated analgesia. The main pharmacokinetic difference between oxycodone and morphine is in oral bioavailability. The bioavailability of oxycodone is >60% and the bioavailability of morphine is 20%. Controlled-release oxycodone is absorbed in a bi-exponential fashion. There is a rapid phase with a mean half-life of 37 min, accounting for 38% of the dose, and a slow phase with a half-life of 6.2 h, which accounts for the residual 62%. Oxycodone elimination is impaired by renal failure because there are both an increased volume of distribution and reduced clearance. A lot of studies prove that the efficacy of controlled-release oxycodone in cancer-pain control is at least the same as morphine, immediate-release oxycodone and hydromorphone. Its toxicity profile seems better than that of morphine. There are actually several illustrations of a lower incidence of side-effects in the central nervous system. It is therefore possible to conclude that oxycodone represents a valid alternative to morphine in the management of moderate to severe cancer pain, also as first-line treatment.
口服阿片类药物是治疗慢性癌痛的首选药物。根据世界卫生组织(WHO)的指南,吗啡是治疗中重度癌痛的首选强阿片类药物。WHO 的这一推荐是基于可用性、临床医生的熟悉程度、已确立的疗效、给药的简单性和相对较低的成本。这并不是基于与其他选择相比具有治疗优势的证据。对于一种阿片类药物治疗后疼痛缓解不足或不能耐受不良反应的患者,通常可以用另一种药物或通过不同途径给予同一种药物进行有效治疗。阿片类药物的转换或改用另一种阿片类药物,有助于一些患者更好地控制疼痛,同时减少相关不良反应。羟考酮是一种μ-阿片受体特异性配体,具有明确的激动剂特性。它是一种有效的强力阿片类药物,在一定程度上也是κ-受体激动剂。与吗啡和其他纯激动剂一样,羟考酮的镇痛作用没有已知的上限。羟考酮的活性代谢物(如羟吗啡酮)可能在羟考酮介导的镇痛中发挥重要作用。羟考酮与吗啡的主要药代动力学差异在于口服生物利用度。羟考酮的生物利用度>60%,而吗啡的生物利用度为 20%。控释羟考酮以双指数方式吸收。有一个快速相,平均半衰期为 37 分钟,占剂量的 38%,一个缓慢相,半衰期为 6.2 小时,占剩余的 62%。肾功能衰竭会损害羟考酮的消除,因为它既有分布容积增加,又有清除率降低。大量研究证明,控释羟考酮在控制癌症疼痛方面的疗效至少与吗啡、即释羟考酮和氢吗啡酮相同。它的毒性谱似乎优于吗啡。实际上,有几项研究表明,在中枢神经系统不良反应的发生率较低。因此,可以得出结论,羟考酮是治疗中重度癌痛的一种有效替代吗啡的药物,也可以作为一线治疗药物。