Okell Lucy C, Drakeley Chris J, Ghani Azra C, Bousema Teun, Sutherland Colin J
Department of Infectious & Tropical Diseases, London School of Hygiene & Tropical Medicine, London, UK.
Malar J. 2008 Jul 9;7:125. doi: 10.1186/1475-2875-7-125.
Artemisinin combination therapies (ACT), which are increasingly being introduced for treatment of Plasmodium falciparum malaria, are more effective against sexual stage parasites (gametocytes) than previous first-line antimalarials and therefore have the potential to reduce parasite transmission. The size of this effect is estimated in symptomatic P. falciparum infections.
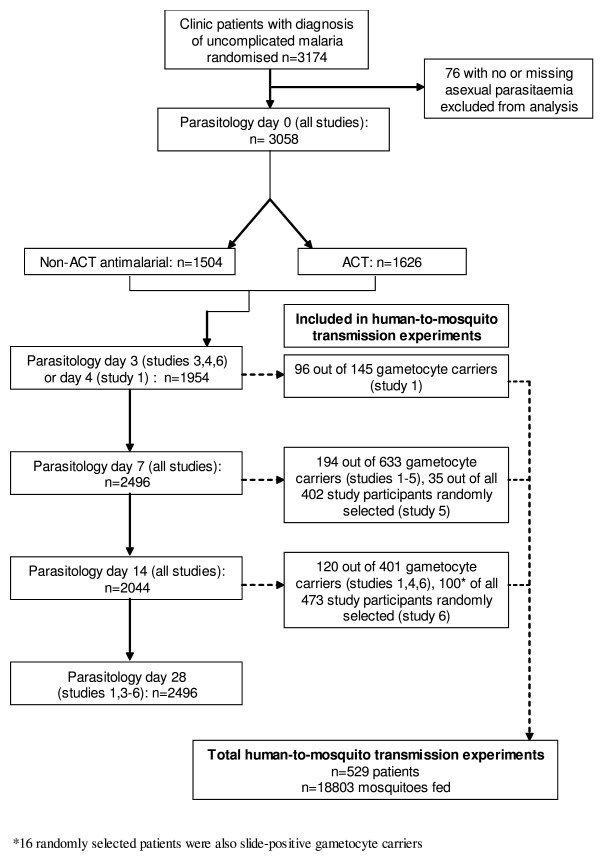
Data on 3,174 patients were pooled from six antimalarial trials conducted in The Gambia and Kenya. Multivariable regression was used to investigate the role of ACT versus non-artemisinin antimalarial treatment, treatment failure, presence of pre-treatment gametocytes and submicroscopic gametocytaemia on transmission to mosquitoes and the area under the curve (AUC) of gametocyte density during the 28 days of follow up.
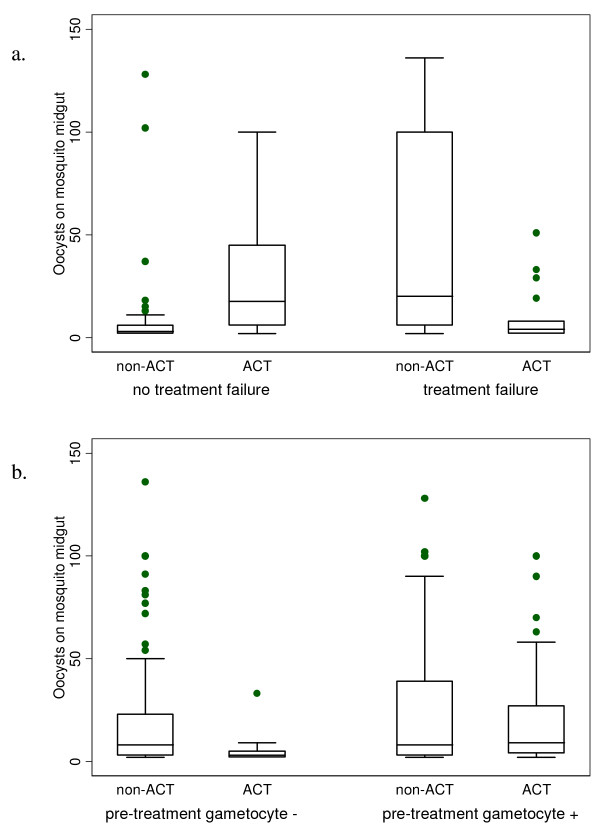
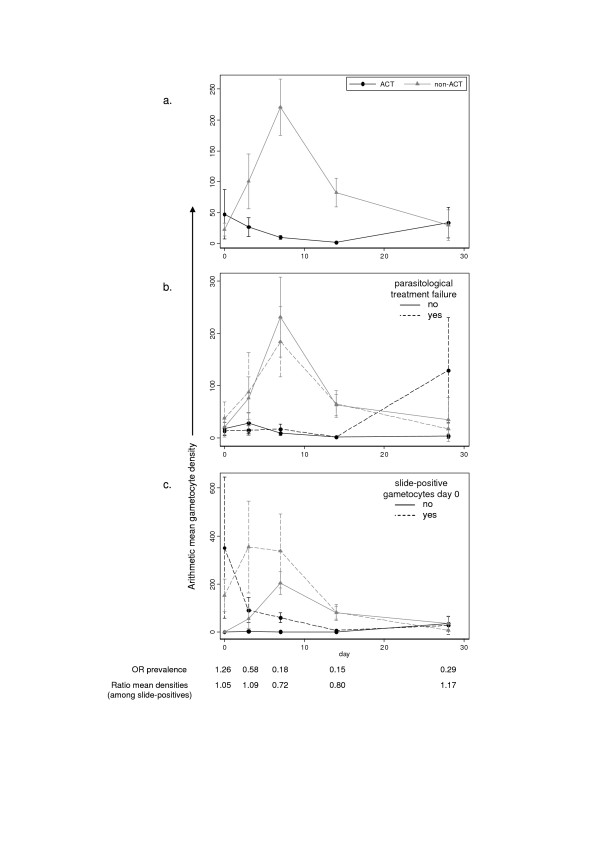
ACT treatment was associated with a significant reduction in the probability of being gametocytaemic on the day of transmission experiments (OR 0.20 95% CI 0.16-0.26), transmission to mosquitoes by slide-positive gametocyte carriers (OR mosquito infection 0.49 95% CI 0.33-0.73) and AUC of gametocyte density (ratio of means 0.35 95% CI 0.31-0.41). Parasitological treatment failure did not account for the difference between ACT and non-artemisinin impact. The presence of slide-positive gametocytaemia prior to treatment significantly reduced ACT impact on gametocytaemia (p < 0.001). Taking account of submicroscopic gametocytaemia reduced estimates of ACT impact in a high transmission setting in Kenya, but not in a lower transmission setting in the Gambia.
Treatment with ACT significantly reduces infectiousness of individual patients with uncomplicated falciparum malaria compared to previous first line treatments. Rapid treatment of cases before gametocytaemia is well developed may enhance the impact of ACT on transmission.
青蒿素联合疗法(ACT)越来越多地被用于治疗恶性疟原虫疟疾,与之前的一线抗疟药物相比,其对有性阶段寄生虫(配子体)更有效,因此有潜力减少寄生虫传播。这种效果的大小是在有症状的恶性疟原虫感染中估计的。
从在冈比亚和肯尼亚进行的六项抗疟试验中汇总了3174例患者的数据。采用多变量回归研究ACT与非青蒿素抗疟治疗、治疗失败、治疗前配子体的存在以及亚显微配子血症对蚊子传播的作用,以及随访28天期间配子体密度曲线下面积(AUC)。
ACT治疗与传播实验当天配子血症的概率显著降低相关(比值比0.20,95%置信区间0.16 - 0.26),玻片阳性配子体携带者向蚊子的传播(比值比蚊子感染0.49,95%置信区间0.33 - 0.73)以及配子体密度的AUC(均值比0.35,95%置信区间0.31 - 0.41)。寄生虫学治疗失败并不能解释ACT和非青蒿素影响之间的差异。治疗前玻片阳性配子血症的存在显著降低了ACT对配子血症的影响(p < 0.001)。考虑亚显微配子血症降低了在肯尼亚高传播环境中ACT影响的估计值,但在冈比亚低传播环境中未降低。
与之前的一线治疗相比,ACT治疗显著降低了单纯性恶性疟患者个体的传染性。在配子血症充分发展之前快速治疗病例可能会增强ACT对传播的影响。