Bejon Philip, Mohammed Shebe, Mwangi Isaiah, Atkinson Sarah H, Osier Faith, Peshu Norbert, Newton Charles R, Maitland Kathryn, Berkley James A
Kenyan Medical Research Institute Centre for Geographic Medicine Research, Kilifi, Kenya.
Am J Clin Nutr. 2008 Dec;88(6):1626-31. doi: 10.3945/ajcn.2008.26510.
Malnutrition is common in the developing world and associated with disease and mortality. Because malnutrition frequently occurs among children in the community as well as those with acute illness, and because anthropometric indicators of nutritional status are continuous variables that preclude a single definition of malnutrition, malnutrition-attributable fractions of admissions and deaths cannot be calculated by simply enumerating individual children.
We determined the malnutrition-attributable fractions among children admitted to a rural district hospital in Kenya, among inpatient deaths and among children with the major causes of severe disease.
We analyzed data from children between 6 and 60 mo of age, comprising 13,307 admissions, 674 deaths, 3068 admissions with severe disease, and 562 community controls by logistic regression, using anthropometric z scores as the independent variable and admission or death as the outcome, to calculate the probability of admission as a result of "true malnutrition" for individual cases. Probabilities were averaged to calculate attributable fractions.
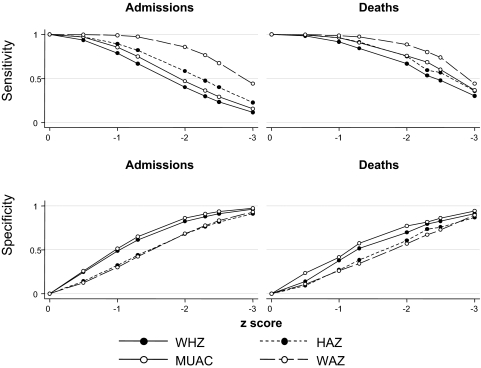
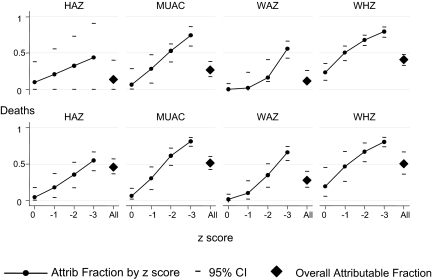
Z scores < -3 were insensitive for malnutrition-attributable deaths and admissions, and no single threshold was both specific and sensitive. The overall malnutrition-attributable fraction for in-hospital deaths was 51% (95% CI: 42%, 61%) with midupper arm circumference. Similar malnutrition-attributable fractions were seen for the major causes of severe disease (severe malaria, gastroenteritis, lower respiratory tract infection, HIV, and invasive bacterial disease).
Despite global improvements, malnutrition still underlies half of the inpatient morbidity and mortality rates among children in rural Kenya. This contribution is underestimated by using conventional clinical definitions of severe malnutrition.
营养不良在发展中国家很常见,且与疾病和死亡率相关。由于营养不良在社区儿童以及急性病患儿中经常出现,而且营养状况的人体测量指标是连续变量,无法对营养不良进行单一界定,因此不能通过简单列举个体儿童来计算营养不良导致的住院率和死亡率。
我们确定了肯尼亚一家农村地区医院收治儿童、住院死亡儿童以及患有严重疾病主要病因的儿童中,营养不良导致的比例。
我们分析了年龄在6至60个月之间儿童的数据,包括13307例住院病例、674例死亡病例、3068例患有严重疾病的住院病例以及562名社区对照儿童。通过逻辑回归分析,将人体测量Z评分作为自变量,住院或死亡作为结果,计算个体病例因“真正营养不良”而住院的概率。对概率进行平均以计算归因比例。
Z评分< -3对于归因于营养不良的死亡和住院情况不敏感,且没有一个单一阈值既具有特异性又具有敏感性。根据上臂中部周长计算,住院死亡中总体营养不良归因比例为51%(95%CI:42%,61%)。对于严重疾病的主要病因(严重疟疾、肠胃炎、下呼吸道感染、艾滋病毒和侵袭性细菌疾病),观察到类似的营养不良归因比例。
尽管全球情况有所改善,但营养不良仍是肯尼亚农村地区儿童住院发病率和死亡率的半数原因。使用传统的严重营养不良临床定义会低估这一影响。